

New ultrasound grading system for cesarean scar pregnancy and its implications for management strategies: An observational cohort study
- PMID: 30092014
- PMCID: PMC6084953
- DOI: 10.1371/journal.pone.0202020
New ultrasound grading system for cesarean scar pregnancy and its implications for management strategies: An observational cohort study
Abstract
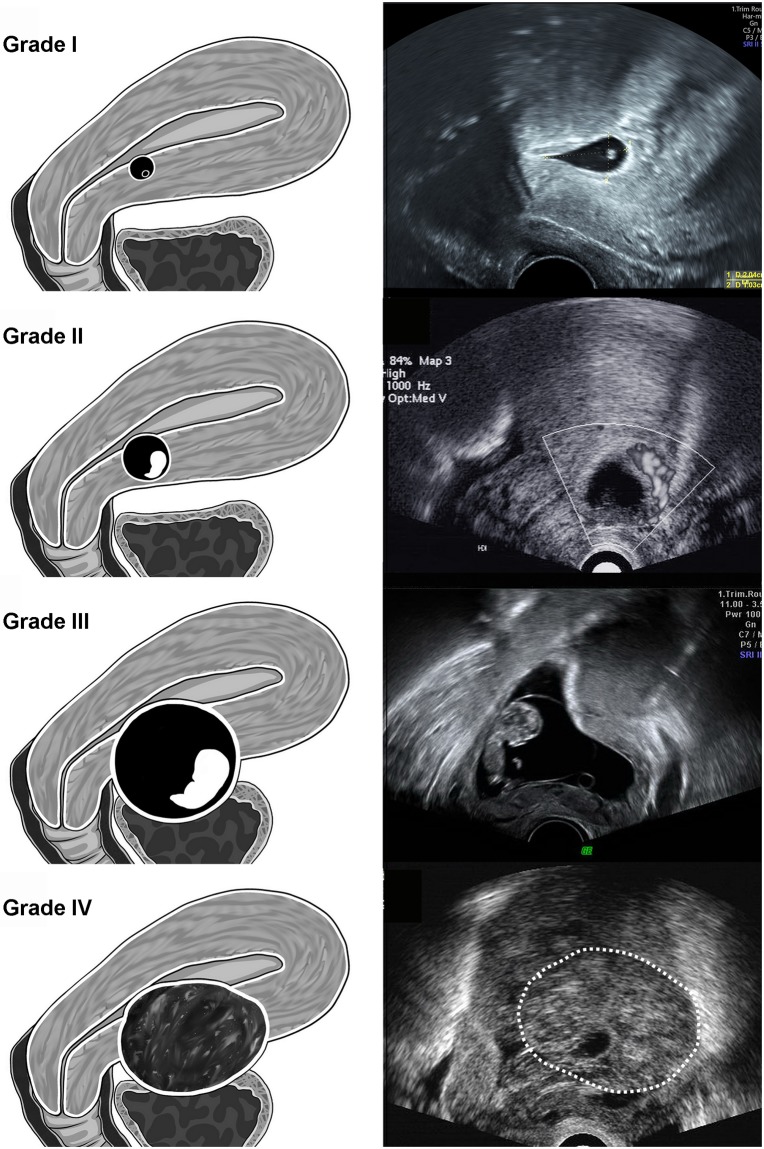
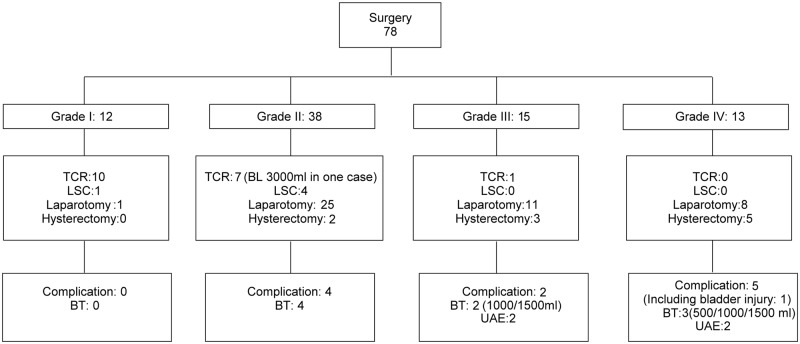
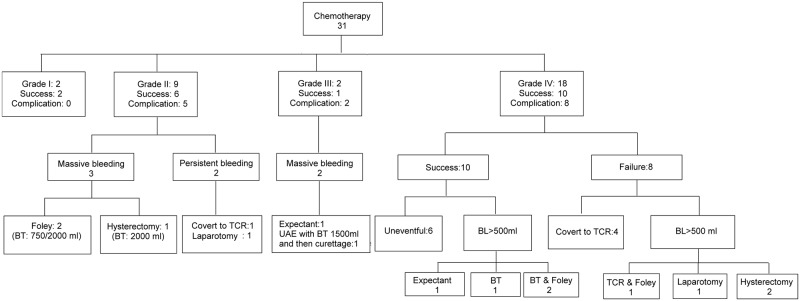
A cesarean section pregnancy (CSP) indicated the gestational sac (GS) implanted in the previous cesarean scar. The clinical manifestations of CSP present a wide range of variations, and the optimal management is yet to be defined. We retrospectively enrolled 109 patients with the diagnosis of CSP from our department and categorized them into four grades based on the ultrasound presentation. Grade I CSP indicated the GS embedded in less than one-half thickness of the lower anterior corpus; and grade II CSP represented the GS extended to more than one-half thickness of overlying myometrium. Grade III CSP implied the GS bulged out of the cesarean scar; and grade IV CSP denoted that GS became an amorphous tumor with rich vascularity at the cesarean scar. Seventy-eight women received surgery, and the complication rate was 14.1% (11/78). Linear regression analysis demonstrated a significant association between the invasiveness of the surgery and their ultrasound gradings. The mainstream operation for grade I CSP was transcervical resection, while the majority of grade III and IV patients required hysterotomy or hysterectomy. Another 31 women received chemotherapy with methotrexate as their initial treatment. The success rate for chemotherapy was 61.3%; the remaining patients required further surgery due to persistent CSP or heavy bleeding during or after chemotherapy. Fifteen patients (48.3%) receiving chemotherapy suffered from complications (mostly bleeding). Among them, 7 (22.6%) patients experienced bleeding of more than 1,000 mL, and 9 (29.0%) of these 31 patients required blood transfusions. Our novel ultrasound grading system for CSP may help to communicate between physicians, and determine the optimal surgical strategy. Chemotherapy with methotrexate for CSP is not satisfactory and is associated with a higher rate of complications.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Transvaginal methotrexate injection for the treatment of cesarean scar pregnancy: efficacy and subsequent fecundity.J Minim Invasive Gynecol. 2014 Sep-Oct;21(5):877-83. doi: 10.1016/j.jmig.2014.03.024. Epub 2014 Apr 14. J Minim Invasive Gynecol. 2014. PMID: 24743111
-
Conservative cesarean scar pregnancy treatment: local methotrexate injection followed by hysteroscopic removal with hysteroscopic tissue removal system.Fertil Steril. 2021 Nov;116(5):1417-1419. doi: 10.1016/j.fertnstert.2021.06.034. Epub 2021 Jul 18. Fertil Steril. 2021. PMID: 34289934
-
[Management of cesarean scar pregnancy by hysteroscopy combined with uterine artery embolism].Zhonghua Fu Chan Ke Za Zhi. 2011 Aug;46(8):591-4. Zhonghua Fu Chan Ke Za Zhi. 2011. PMID: 22169517 Chinese.
-
Ectopic pregnancies in caesarean section scars: 5 years experience.Clin Imaging. 2020 Oct;66:26-34. doi: 10.1016/j.clinimag.2020.04.037. Epub 2020 May 3. Clin Imaging. 2020. PMID: 32442857 Review.
-
Local Methotrexate Injection as the First-line Treatment for Cesarean Scar Pregnancy: Review of the Literature.J Minim Invasive Gynecol. 2015 Jul-Aug;22(5):753-8. doi: 10.1016/j.jmig.2015.04.008. Epub 2015 Apr 15. J Minim Invasive Gynecol. 2015. PMID: 25889882 Review.
Cited by
-
Cesarean Scar Pregnancy Successfully Managed to Term: When the Patient Is Determined to Keep the Pregnancy.Medicina (Kaunas). 2020 Sep 24;56(10):496. doi: 10.3390/medicina56100496. Medicina (Kaunas). 2020. PMID: 32987706 Free PMC article.
-
Definition and sonographic reporting system for Cesarean scar pregnancy in early gestation: modified Delphi method.Ultrasound Obstet Gynecol. 2022 Apr;59(4):437-449. doi: 10.1002/uog.24815. Ultrasound Obstet Gynecol. 2022. PMID: 34779085 Free PMC article.
-
A comparison between laparoscopy and hysteroscopy approach in treatment of cesarean scar pregnancy.Medicine (Baltimore). 2020 Oct 23;99(43):e22845. doi: 10.1097/MD.0000000000022845. Medicine (Baltimore). 2020. PMID: 33120815 Free PMC article.
-
A scoring system predicts the adverse outcomes for cesarean scar pregnancy treated with transvaginal hysterotomy.Quant Imaging Med Surg. 2025 Jun 6;15(6):5086-5100. doi: 10.21037/qims-24-1337. Epub 2025 Jun 3. Quant Imaging Med Surg. 2025. PMID: 40606340 Free PMC article.
-
Pituitrin Injection before Hysteroscopic Curettage for Treating Type I Cesarean Scar Pregnancy in Comparison with Uterine Artery Embolization: A Retrospective Study.J Obstet Gynaecol India. 2023 Jun;73(3):229-234. doi: 10.1007/s13224-022-01724-w. Epub 2022 Dec 18. J Obstet Gynaecol India. 2023. PMID: 37324364 Free PMC article.
References
-
- Pekar-Zlotin M, Melcer Y, Levinsohn-Tavor O, Tovbin J, Vaknin Z, Maymon R. Cesarean Scar Pregnancy and Morbidly Adherent Placenta: Different or Similar? Isr Med Assoc J. 2017;19(3):168–71. Epub 2017/05/01. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
