

Coronary Microvascular Dysfunction and Cardiovascular Risk in Obese Patients
- PMID: 30092946
- PMCID: PMC6592712
- DOI: 10.1016/j.jacc.2018.05.049
Coronary Microvascular Dysfunction and Cardiovascular Risk in Obese Patients
Abstract
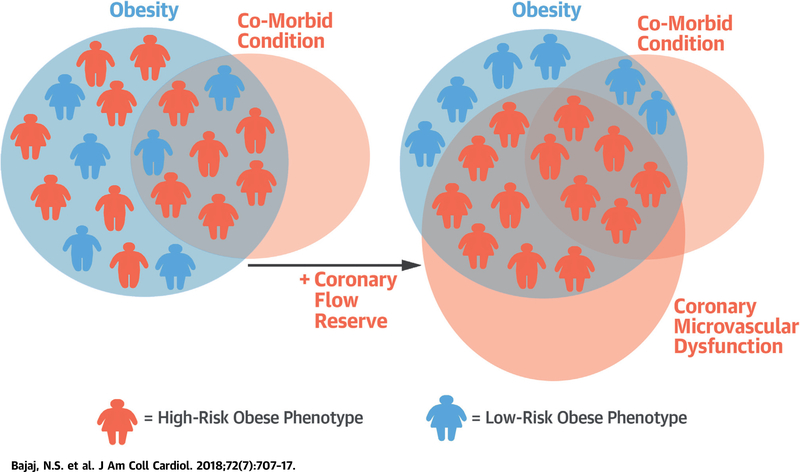
Background: Besides body mass index (BMI), other discriminators of cardiovascular risk are needed in obese patients, who may or may not undergo consideration for bariatric surgery. Coronary microvascular dysfunction (CMD), defined as impaired coronary flow reserve (CFR) in the absence of flow-limiting coronary artery disease, identifies patients at risk for adverse events independently of traditional risk factors.
Objectives: The study sought to investigate the relationship among obesity, CMD, and adverse outcomes.
Methods: Consecutive patients undergoing evaluation for coronary artery disease with cardiac stress positron emission tomography demonstrating normal perfusion (N = 827) were followed for median 5.6 years for events, including death and hospitalization for myocardial infarction or heart failure.
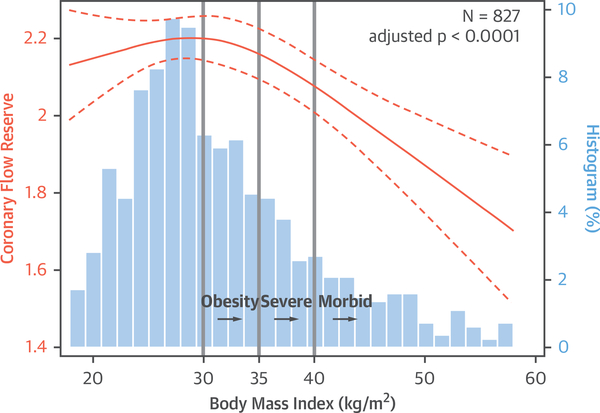
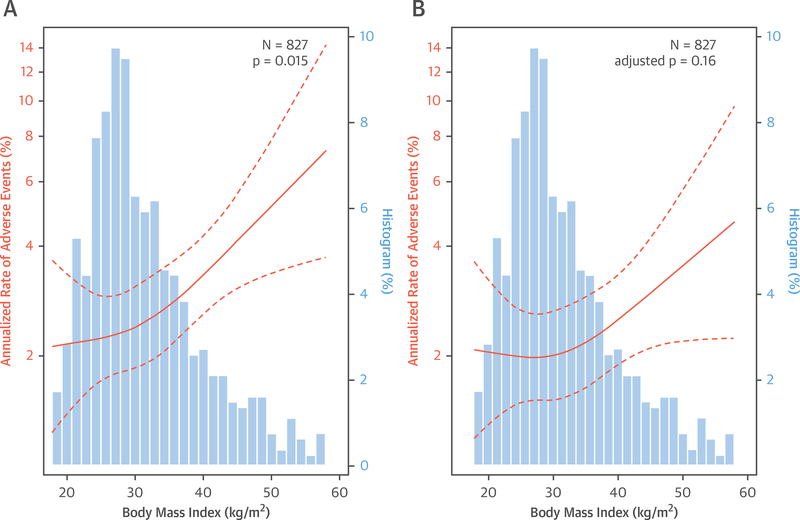
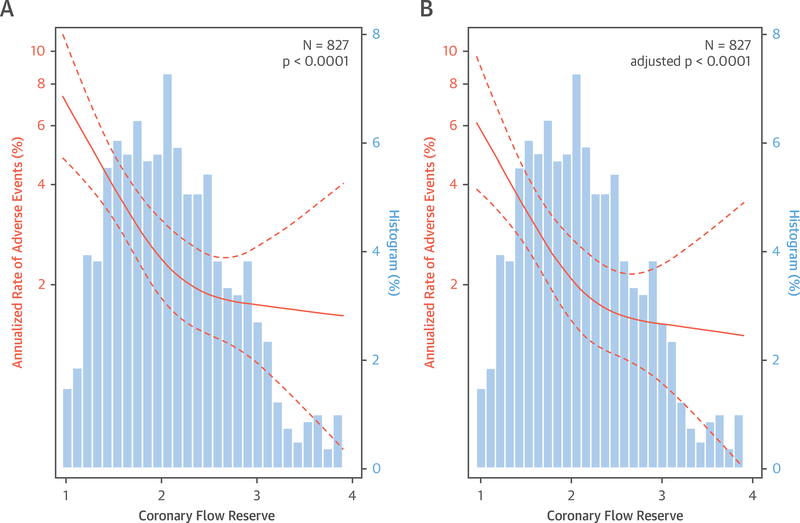
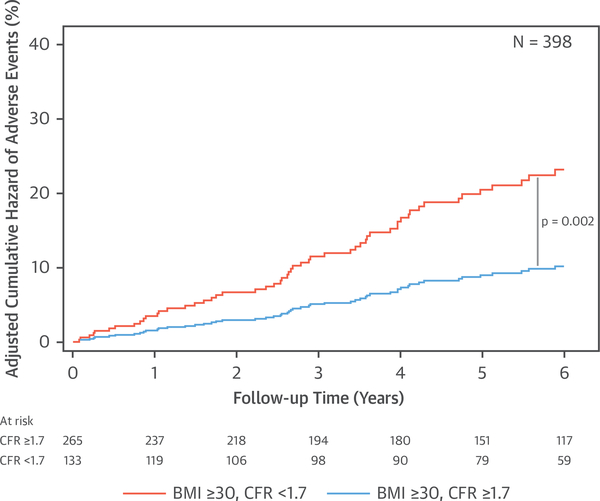
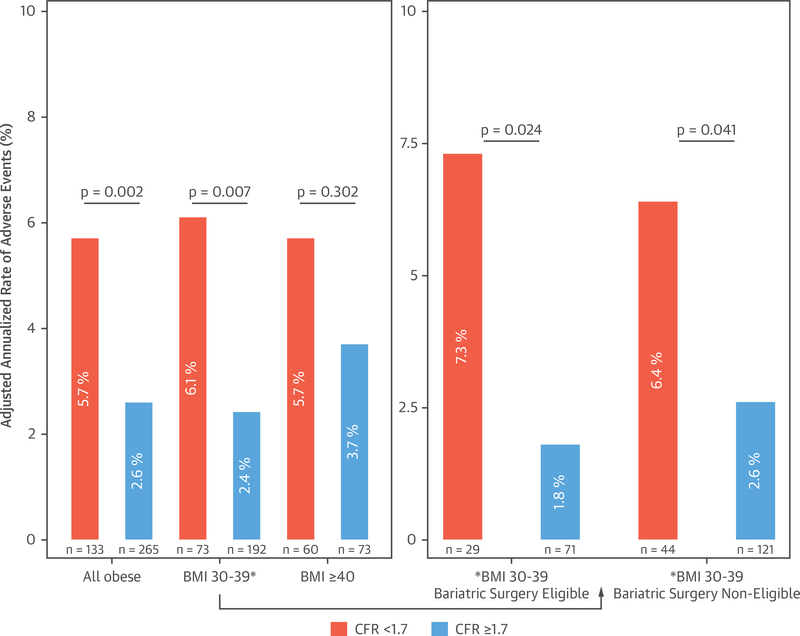
Results: An inverted independent J-shaped relationship was observed between BMI and CFR, such that in obese patients CFR decreased linearly with increasing BMI (adjusted p < 0.0001). In adjusted analyses, CFR but not BMI remained independently associated with events (for a 1-U decrease in CFR, adjusted hazard ratio: 1.95; 95% confidence interval: 1.41 to 2.69; p < 0.001; for a 10-U increase in BMI, adjusted hazard ratio: 1.20; 95% confidence interval: 0.95 to 1.50; p = 0.125) and improved model discrimination (C-index 0.71 to 0.74). In obese patients, individuals with impaired CFR demonstrated a higher adjusted rate of events (5.7% vs. 2.6%; p = 0.002), even in those not currently meeting indications for bariatric surgery (6.4% vs. 2.6%; p = 0.04).
Conclusions: In patients referred for testing, CMD was independently associated with elevated BMI and adverse outcomes, and was a better discriminator of risk than BMI and traditional risk factors. CFR may facilitate management of obese patients beyond currently used markers of risk.
Keywords: bariatric surgery; body mass index; coronary microvascular dysfunction; obesity; prognosis.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Coronary Microvascular Dysfunction: A Preferred Risk Marker in Obesity?J Am Coll Cardiol. 2018 Aug 14;72(7):718-720. doi: 10.1016/j.jacc.2018.05.050. J Am Coll Cardiol. 2018. PMID: 30092947 No abstract available.
References
-
- Heymsfield SB, Wadden TA. Mechanisms, pathophysiology, and management of obesity. N Engl J Med 2017;376:254–66. - PubMed
-
- Ortega FB, Lavie CJ, Blair SN. Obesity and cardiovascular disease. Circ Res 2016;118:1752–70. - PubMed
-
- Stefan N, Haring HU, Hu FB, Schulze MB. Metabolically healthy obesity: epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol 2013;1:152–62. - PubMed
-
- Kim J, Eisenberg D, Azagury D, Rogers A, Campos GM. American Society for Metabolic and Bariatric Surgery position statement on long-term survival benefit after metabolic and bariatric surgery. Surg Obes Relat Dis 2016;12:453–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
