

Comparison between transoral laser surgery and radiotherapy in the treatment of early glottic cancer: A systematic review and meta-analysis
- PMID: 30093659
- PMCID: PMC6085327
- DOI: 10.1038/s41598-018-30218-x
Comparison between transoral laser surgery and radiotherapy in the treatment of early glottic cancer: A systematic review and meta-analysis
Abstract
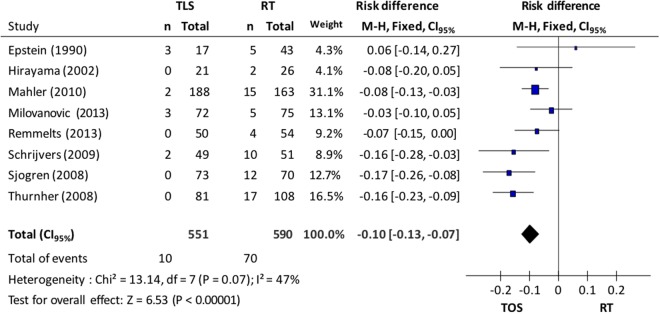
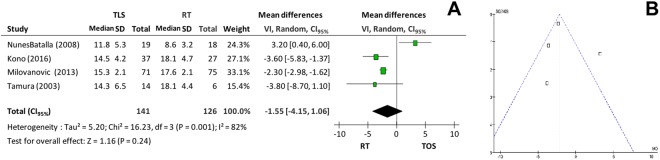
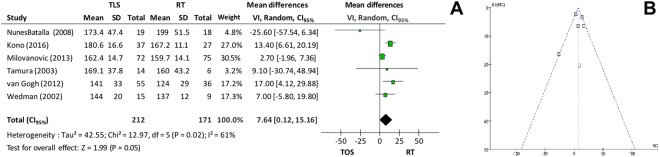
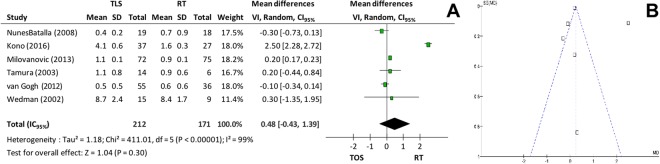
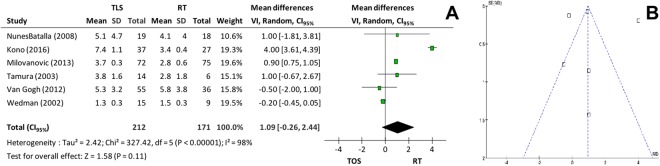
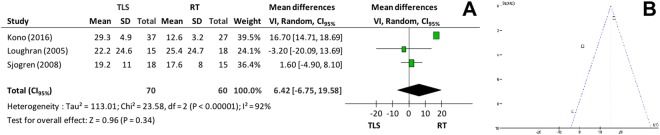
A therapeutic decision in the treatment of Tis/T1a glottic carcinoma with radiotherapy (RT) or transoral laser surgery (TOS) is still an open issue. Oncologic outcome and voice quality may support the choice for the latter To conduct a systematic review and meta-analysis to compare oncologic and functional outcomes of TOS and RT as treatment options for Tis/T1a glottic cancer. Literature research on online databases was carried out. Potentially eligible articles were reviewed. Relevant articles were selected and evaluated. There was statistical significance favoring patients initially treated with TOS when it comes to overall survival, disease-specific survival and larynx preservation. No difference in local control was found. TMF, Jitter and Shimmmer measurements presented statistically significant results in favor of RT. Self-assessment of voice quality (VHI) and f0 showed no statistically significant differences. Maximum Phonation Time (MPT) had a better response to RT. There is a trend in favor of RT. Tis/T1a glottic cancer patients submitted to TOS had significant overall and disease specific survival and had fewer risks of having a total laryngectomy, when compared to the radiotherapy group. The self-assessment of voice quality and f0 did not show any difference; however, Jitter, Shimmer and MPT measurements favored radiotherapy.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Al-Mamgani A, et al. Radiotherapy for T1-2N0 glottic cancer: a multivariate analysis of predictive factors for the long-term outcome in 1050 patients and a prospective assessment of quality of life and voice handicap index in a subset of 233 patients. Clin Otolaryngol. 2013;38:306–312. doi: 10.1111/coa.12139. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
