

Imaging modalities for temporomandibular joint disorders: an update
- PMID: 30093805
- PMCID: PMC6082607
- DOI: 10.15386/cjmed-970
Imaging modalities for temporomandibular joint disorders: an update
Abstract
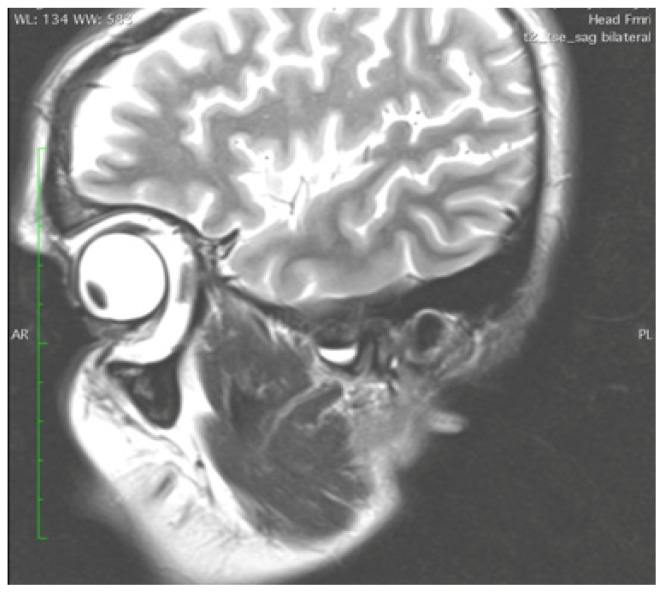
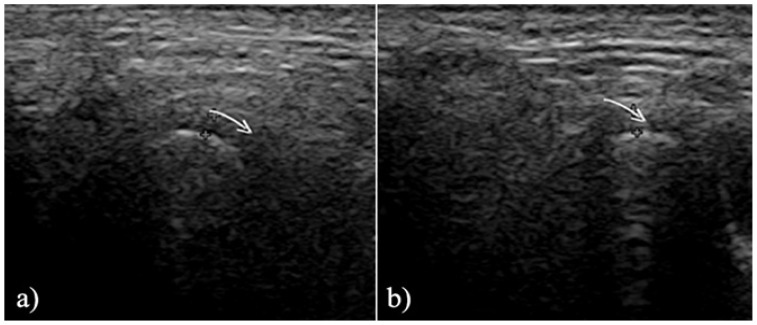
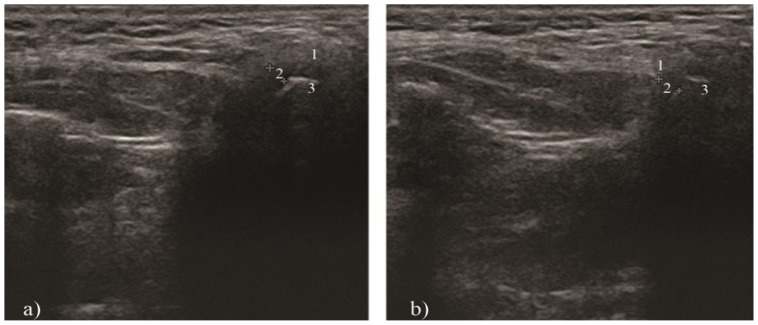
The diagnosis and management of temporomandibular disorders (TMD) require both clinical and imaging examinations of the temporomandibular joint (TMJ). A variety of modalities can be used to image the TMJ, including magnetic resonance imaging (MRI), computed tomography (CT), cone beam CT, ultrasonography, conventional radiography. The present review outlines the indications of the most frequently used imaging techniques in TMD diagnosis. Because of the anatomic complexity of the TMJ, imaging can be difficult. Choosing the proper imaging technique is essential. Conventional radiography, nowadays, is of limited interest. The use of flat plane films for TMJ pathology is not sufficient, because this joint requires three dimensional imaging views. Osseous changes are better visualized with CT and cone beam CT. Cone beam CT provides high-resolution multiplanar reconstruction of the TMJ, with a low radiation dose, without superimposition of the bony structures. MRI is a noninvasive technique, considered to be the gold standard in imaging the soft tissue components of the TMJ. MRI is used to evaluate the articular disc in terms of location and morphology. Moreover, the early signs of TMD and the presence of joint effusion can be determined. High-resolution ultrasonography is a noninvasive, dynamic, inexpensive imaging technique, which can be useful in diagnosing TMJ disc displacements. The diagnostic value of high-resolution ultrasonography is strictly dependent on the examiner's skills and on the equipment used.
Keywords: computed tomography; magnetic resonance imaging; temporomandibular disorders; temporomandibular joint; ultrasonography.
Figures

References
-
- Okeson JP. Management of temporomandibular disorders and occlusion. 6th ed. St. Louis: Mosby; 2008. pp. 5–21.
-
- Slavicek R. The masticatory organ: functions and dysfunctions. Gamma Meidizinisch-wissenschaftliche Forbildungs- GmbH; Klostenburg: 2006. pp. 60–66.
-
- Alomar X, Medrano J, Cabratosa J, Clavero JA, Lorente M, Serra I, et al. Anatomy of the temporomandibular joint. Semin Ultrasound CT MR. 2007;28(3):170–183. - PubMed
-
- De Leeuw R, Klasser G. Orofacial Pain: Guidelines for assessement, diagnosis and management. 5th ed. Chicago: Quintessence Publishing Co., Inc; 2013. pp. 127–137.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources