

Use of lung-protective strategies during one-lung ventilation surgery: a multi-institutional survey
- PMID: 30094255
- PMCID: PMC6064789
- DOI: 10.21037/atm.2018.06.02
Use of lung-protective strategies during one-lung ventilation surgery: a multi-institutional survey
Abstract
Background: Limited evidence suggests that intraoperative lung-protective ventilation (LPV) during one-lung ventilation (OLV) may reduce respiratory complications after thoracic surgery. Little is known about LPV practices during OLV. Our purpose was to assess the state of practice/perspectives of anesthesiologists regarding LPV during elective OLV.
Methods: We conducted a multi-institutional cross-sectional survey of anesthesiologists performing OLV at high-volume Canadian tertiary/university centers. The survey was designed, refined and distributed by a multi-disciplinary team using the Dillman method. Univariable and multivariable analyses were used.
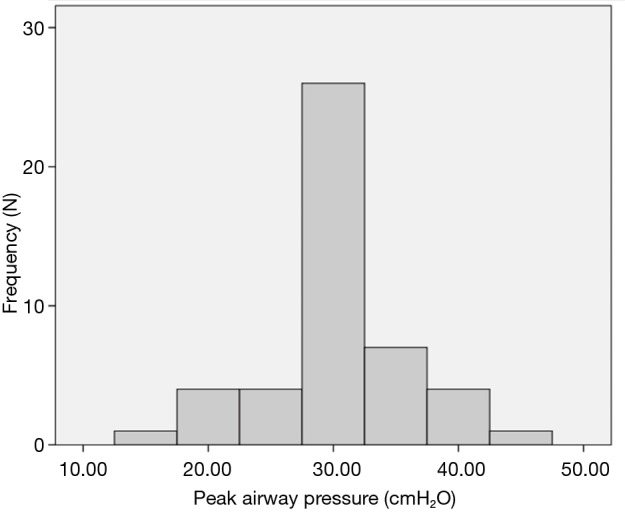
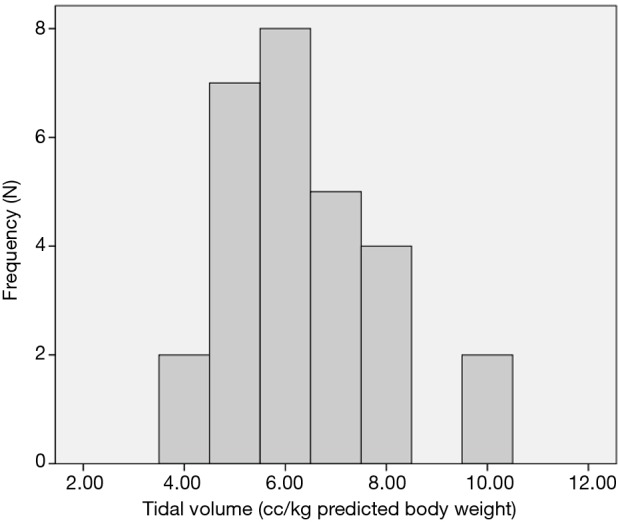
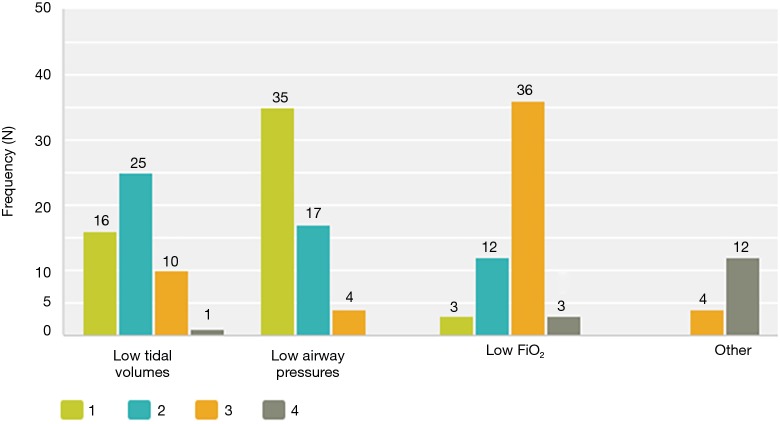
Results: Seventy-five (63%) of 120 eligible respondents completed the survey. Although the critical care literature focuses on minimizing tidal volume (TV) as the central strategy of LPV, most respondents (89%, n=50/56) focused on minimizing peak airway pressure (PAP) as their primary strategy of intraoperative LPV. Only 64% (n=37/58) reported actively trying to minimize TV. While 32% (n=17/54) were unsure about the current evidence regarding LPV, 67% (n=36/54) believed that the evidence favoured their use during OLV. Perceived clinical and institutional barriers were the only predictors of reduced attempts to minimize TV on univariate analyses. In multivariable/adjusted analyses, perceived institutional barriers were the only predictors of reduced attempts to minimize TV with adjusted odds ratio of 0.1 (95% CI: 0.03-0.6).
Conclusions: Most anesthesiologists defined low PAP as the primary strategy of LPV during OLV and attempted to minimize it. This study is the first to assess the practice/perspectives of anesthesiologists regarding LPV during OLV and also the first to explore predictors of LPV use. Randomized trials are currently ongoing. However, this study suggests that institutional barriers may subvert future knowledge translation and need to be addressed.
Keywords: Acute respiratory distress syndrome (ARDS); anesthesia; lung physiology; perioperative care.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Meade MO, Cook DJ, Guyatt GH, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2008;299:637-45. 10.1001/jama.299.6.637 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials