

Detrimental Outcomes of Unmasking Cryptococcal Meningitis With Recent ART Initiation
- PMID: 30094292
- PMCID: PMC6080052
- DOI: 10.1093/ofid/ofy122
Detrimental Outcomes of Unmasking Cryptococcal Meningitis With Recent ART Initiation
Abstract
Background: Increased antiretroviral therapy (ART) availability has been associated with more patients developing cryptococcosis after ART initiation. Despite this changing epidemiology, data regarding cryptococcal meningitis in those already receiving ART are limited. We compared clinical presentations and outcomes among ART-naïve and ART-experienced Ugandans.
Methods: We prospectively enrolled 605 HIV-infected persons with first-episode cryptococcal meningitis from August 2013 to May 2017 who received amphotericin-based combination therapy. We classified participants by ART status and ART duration and compared groups for 2-week survival.
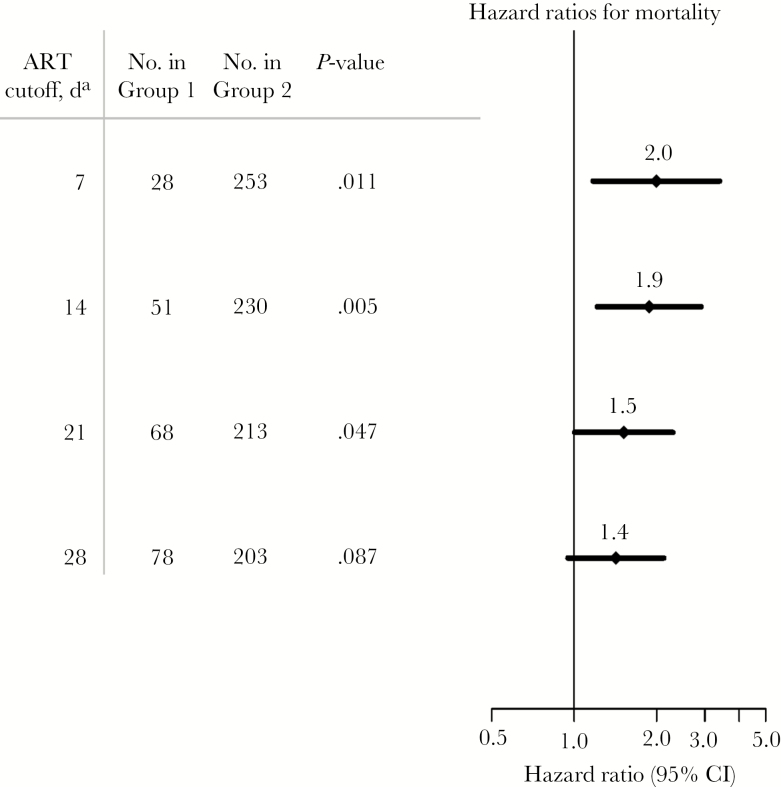
Results: Overall, 46% (281/605) of participants were receiving ART at presentation. Compared with those not receiving ART, those receiving ART had higher CD4 counts (P < .001) and lower cerebrospinal fluid fungal burdens (P < .001). Of those receiving ART, 56% (156/281) initiated ART within 6 months, and 18% (51/281) initiated ART within 14 days. Two-week mortality did not differ by ART status (27% in both ART-naïve and ART-experienced%; P > .99). However, 47% (24/51) of those receiving ART for ≤14 days died within 2 weeks, compared with 19% (20/105) of those receiving ART for 15-182 days and 26% (32/125) of those receiving ART for >6 months (P < .001). Among persons receiving ART for >6 months, 87% had HIV viral loads >1000 copies/mL.
Conclusions: Cryptococcosis after ART initiation is common in Africa. Patients initiating ART who unmask cryptococcal meningitis are at a high risk of death. Immune recovery in the setting of central nervous system infection is detrimental, and management of this population requires further study. Implementing pre-ART cryptococcal antigen screening is urgently needed to prevent cryptococcal meningitis after ART initiation.
Keywords: HIV; antiretroviral therapy; cryptococcal meningitis; cryptococcus; immune reconstitution inflammatory syndrome.
Figures


References
-
- Mfinanga S, Chanda D, Kivuyo SL, et al. . REMSTART trial team Cryptococcal meningitis screening and community-based early adherence support in people with advanced HIV infection starting antiretroviral therapy in Tanzania and Zambia: an open-label, randomised controlled trial. Lancet 2015; 385:2173–82. - PubMed
-
- Kaplan JE, Vallabhaneni S, Smith RM, et al. . Cryptococcal antigen screening and early antifungal treatment to prevent cryptococcal meningitis: a review of the literature. J Acquir Immune Defic Syndr 2015; 68(Suppl 3):S331–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
