

Transition to universal primary health care coverage in Brazil: Analysis of uptake and expansion patterns of Brazil's Family Health Strategy (1998-2012)
- PMID: 30096201
- PMCID: PMC6086633
- DOI: 10.1371/journal.pone.0201723
Transition to universal primary health care coverage in Brazil: Analysis of uptake and expansion patterns of Brazil's Family Health Strategy (1998-2012)
Erratum in
-
Correction: Transition to universal primary health care coverage in Brazil: Analysis of uptake and expansion patterns of Brazil's Family Health Strategy (1998-2012).PLoS One. 2021 May 11;16(5):e0251764. doi: 10.1371/journal.pone.0251764. eCollection 2021. PLoS One. 2021. PMID: 33974650 Free PMC article.
Abstract
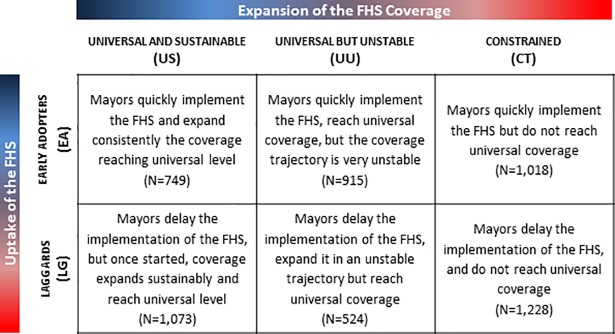
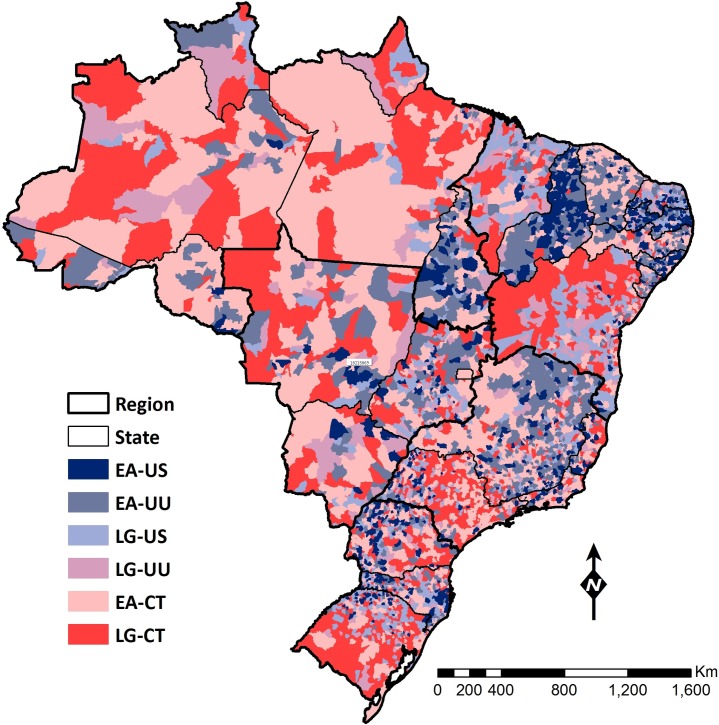
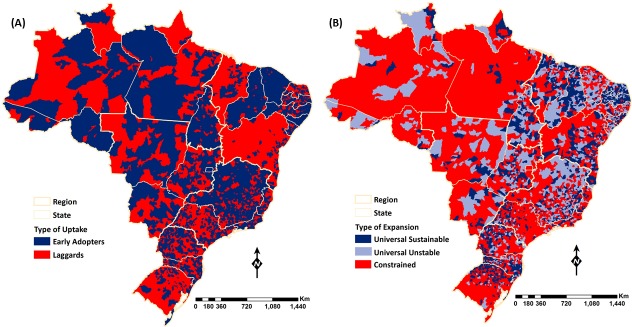
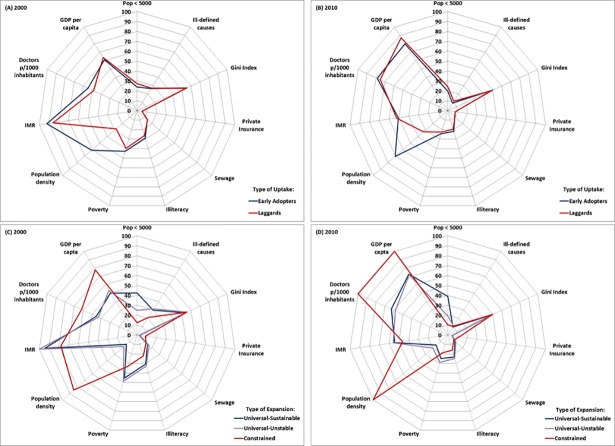
Family Health Strategy, the primary health care program in Brazil, has been scaled up throughout the country, but its expansion has been heterogeneous across municipalities. We investigate if there are unique municipal characteristics that can explain the timing of uptake and the pattern of expansion of the Family Health Strategy from years 1998 to 2012. We categorized municipalities in six groups based on the relative speed of the Family Health Strategy uptake and the pattern of Family Health Strategy coverage expansion. We assembled data for 11 indicators for years 2000 and 2010, for 5,507 municipalities, and assessed differences in indicators across the six groups, which we mapped to examine spatial heterogeneities. Important factors differentiating early and late adopters of the Family Health Strategy were supply of doctors and population density. Sustained coverage expansion was related mainly to population size, marginal benefits of the program and doctors' supply. The uptake was widespread nationwide with no distinct patterns among regions, but highly heterogeneous at the state and municipal level. The Brazilian experience of expanding primary health care offers three lessons in relation to factors influencing diffusion of primary health care. First, the funding mechanism is critical for program implementation, and must be accompanied by ways to support the supply of primary care physicians in low density areas. Second, in more developed and bigger areas the main challenge is lack of incentives to pursue universal coverage, especially due to the availability of private insurance. Third, population size is a crucial element to guarantee coverage sustainability over time.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. Health in 2015: from MDGs, Millennium Development Goals to SDGs, Sustainable Development Goals Geneva: World Health Organization, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
