

Mechanical dilatation of the cervix during elective caeserean section before the onset of labour for reducing postoperative morbidity
- PMID: 30096215
- PMCID: PMC6513223
- DOI: 10.1002/14651858.CD008019.pub3
Mechanical dilatation of the cervix during elective caeserean section before the onset of labour for reducing postoperative morbidity
Abstract
Background: During elective (planned) caesarean sections, some obstetricians routinely dilate the cervix intraoperatively, using sponge forceps, a finger, or other instruments, because the cervix of women not in labour may not be dilated, and this may cause obstruction of blood or lochia drainage. However, mechanical cervical dilatation during caesarean section may result in contamination by vaginal micro-organisms during dilatation, and increase the risk of infection or cervical trauma.
Objectives: To determine the effects of mechanical dilatation of the cervix during elective caesarean section on postoperative morbidity.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register, ClinicalTrials.gov, the WHO International Clinical Trials Registry Platform (ICTRP) and reference lists of retrieved studies on 20 September 2017.
Selection criteria: We included all randomised, quasi-randomised, and cluster-randomised controlled trials comparing intraoperative cervical dilatation using a finger, sponge forceps, or other instruments during elective caesarean section versus no mechanical dilatation.
Data collection and analysis: Two review authors independently assessed trials for inclusion and risk of bias, extracted data and checked them for accuracy. We assessed the quality of the evidence using the GRADE approach.
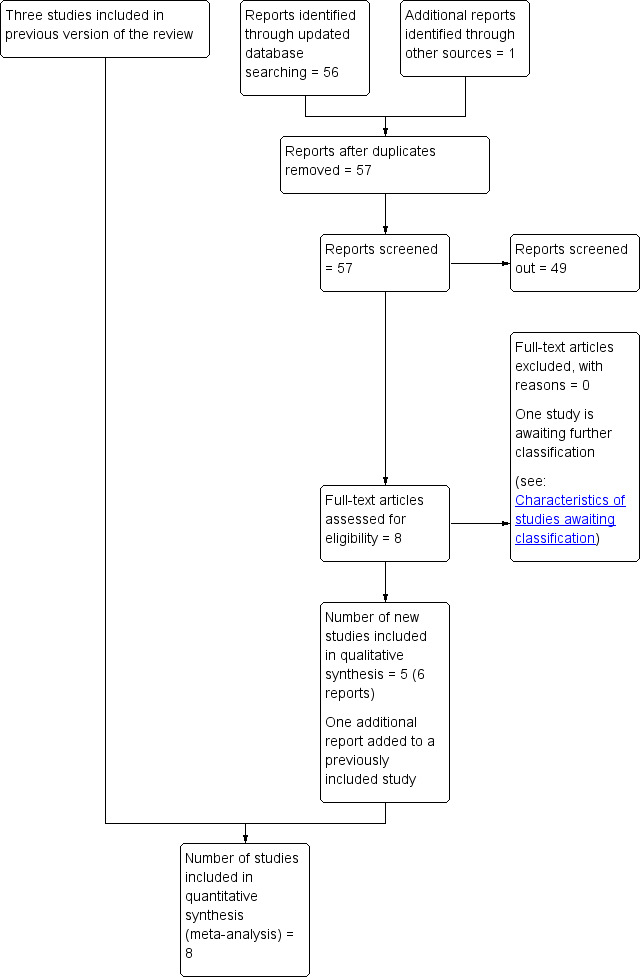
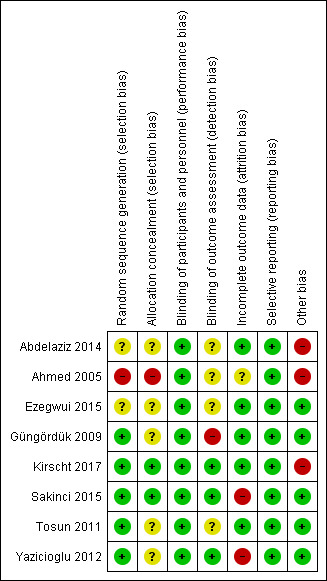
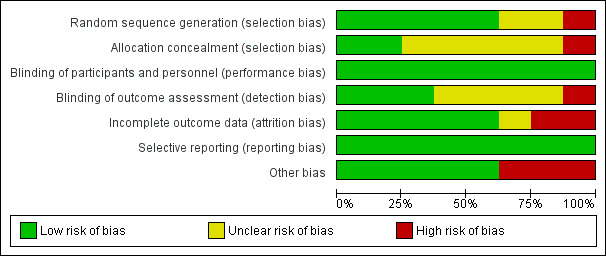
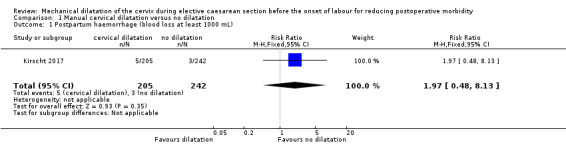
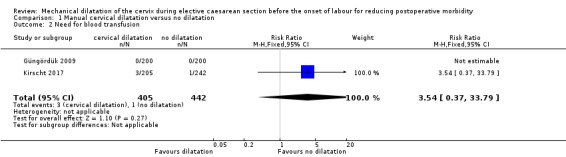
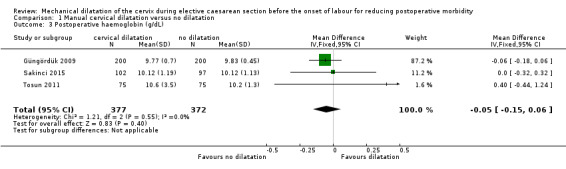
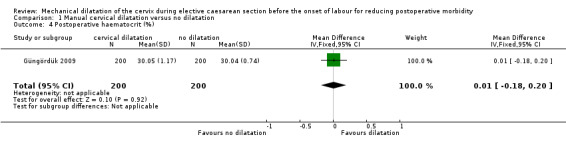
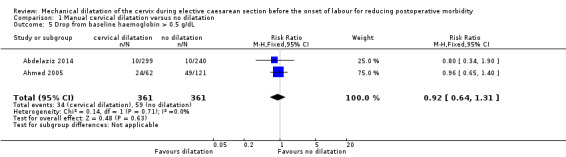
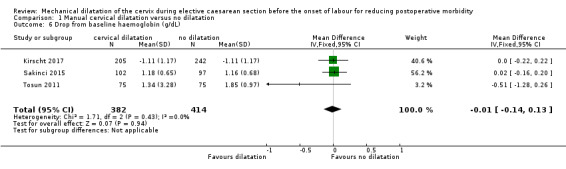
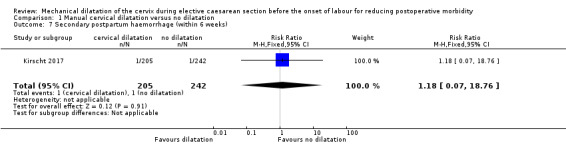
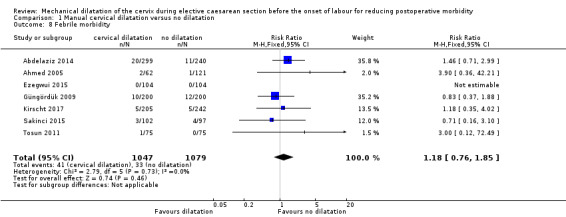
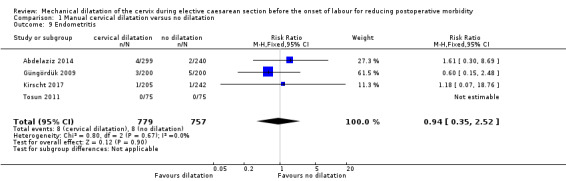
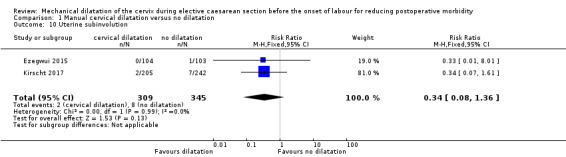
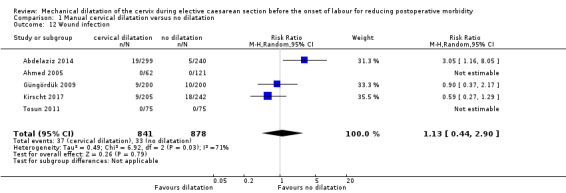
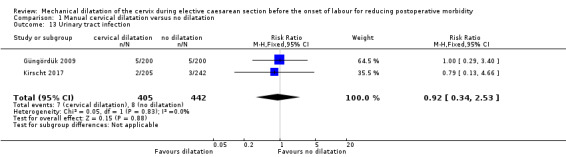
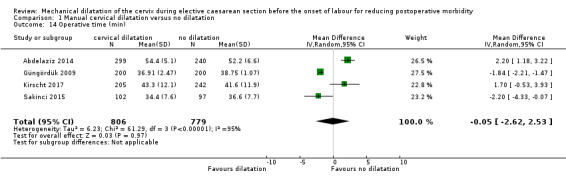
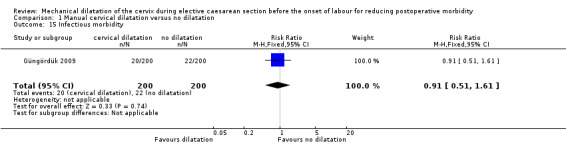
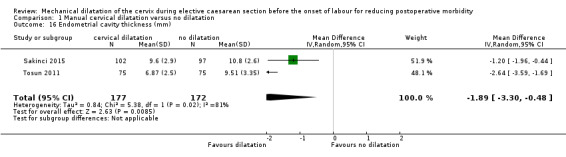
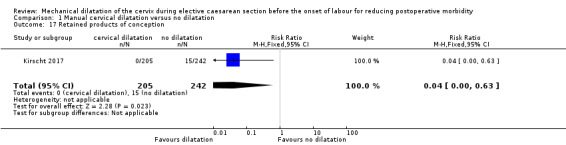
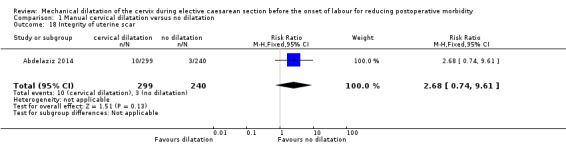
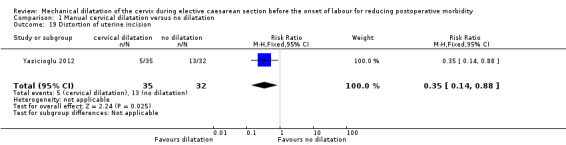
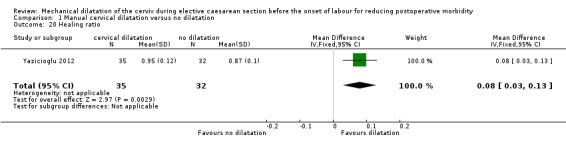
Main results: We included eight studies with a total of 2227 women undergoing elective caesarean section. Of these, 1097 underwent intraoperative cervical dilatation with a double-gloved index finger or Hegar dilator inserted into the cervical canal to dilate, and 1130 did not undergo intraoperative cervical dilatation. Six of the eight included trials had high risk of bias for some of the risk of bias domains.Very low-quality evidence suggested it was unclear whether cervical dilatation had any impact on postpartum haemorrhage (estimated blood loss greater than 1000 mL; risk ratio (RR) 1.97, 95% confidence interval (CI) 0.48 to 8.13; 5/205 versus 3/242; one study, 447 women).Low- or very low-quality evidence showed no clear difference for the need for blood transfusion (RR 3.54, 95% CI 0.37 to 33.79; two studies, 847 women); postoperative haemoglobin (mean difference (MD -0.05, 95% CI -0.15 to 0.06; three studies, 749 women), or haematocrit (MD 0.01%, 95% CI -0.18 to 0.20; one study, 400 women); the incidence of drop from baseline haemoglobin above 0.5 g/dL (RR 0.92, 95% CI 0.64 to 1.31; two studies, 722 women), or amount of haemoglobin drop (MD -0.01 g/dL, 95% -0.14 to 0.13; three studies, 796 women); the incidence of secondary postpartum haemorrhage within six weeks (RR 1.18, 95% CI 0.07 to 18.76; one study, 447 women); febrile morbidity (RR 1.18, 95% CI 0.76 to 1.85; seven studies, 2126 women); endometritis (RR 0.94, 95% CI 0.35 to 2.52; four studies, 1536 women); or uterine subinvolution (RR 0.34, 95% CI 0.08 to 1.36; two studies, 654 women); the results crossed the line of no effect for all of the outcomes. There were no data for cervical trauma.We found a slight improvement with mechanical dilatation for these secondary outcomes, not prespecified in the protocol: mean blood loss, endometrial cavity thickness, retained products of conception, distortion of uterine incision, and healing ratio. The evidence for these outcomes was based on one or two studies. Cervical dilatation did not have a clear effect on these secondary outcomes, not prespecified in the protocol: wound infection, urinary tract infection, operative time, infectious morbidity, and integrity of uterine scar.
Authors' conclusions: At this time, the evidence does not support or refute the use of mechanical dilatation of the cervix during elective caesarean section for reducing postoperative morbidity.Further large, well-designed studies are required to compare the effect of intraoperative mechanical dilatation of the cervix with no intraoperative mechanical cervical dilatation for reducing postoperative morbidity.
Conflict of interest statement
Tippawan Liabsuetrakul: none known
Krantarat Peeyananjarassri: none known
Figures

Update of
-
Mechanical dilatation of the cervix at non-labour caesarean section for reducing postoperative morbidity.Cochrane Database Syst Rev. 2011 Nov 9;(11):CD008019. doi: 10.1002/14651858.CD008019.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2018 Aug 10;8:CD008019. doi: 10.1002/14651858.CD008019.pub3. PMID: 22071843 Updated.
Similar articles
-
Mechanical dilatation of the cervix at non-labour caesarean section for reducing postoperative morbidity.Cochrane Database Syst Rev. 2011 Nov 9;(11):CD008019. doi: 10.1002/14651858.CD008019.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2018 Aug 10;8:CD008019. doi: 10.1002/14651858.CD008019.pub3. PMID: 22071843 Updated.
-
Skin preparation for preventing infection following caesarean section.Cochrane Database Syst Rev. 2020 Jun 25;6(6):CD007462. doi: 10.1002/14651858.CD007462.pub5. Cochrane Database Syst Rev. 2020. PMID: 32580252 Free PMC article.
-
Skin preparation for preventing infection following caesarean section.Cochrane Database Syst Rev. 2018 Oct 22;10(10):CD007462. doi: 10.1002/14651858.CD007462.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Jun 25;6:CD007462. doi: 10.1002/14651858.CD007462.pub5. PMID: 30346040 Free PMC article. Updated.
-
Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections.Cochrane Database Syst Rev. 2020 Apr 26;4(4):CD007892. doi: 10.1002/14651858.CD007892.pub7. Cochrane Database Syst Rev. 2020. PMID: 32335895 Free PMC article.
-
Interventions for preventing nausea and vomiting in women undergoing regional anaesthesia for caesarean section.Cochrane Database Syst Rev. 2021 May 18;5(5):CD007579. doi: 10.1002/14651858.CD007579.pub3. Cochrane Database Syst Rev. 2021. PMID: 34002866 Free PMC article.
Cited by
-
The Case for Standardizing Cesarean Delivery Technique: Seeing the Forest for the Trees.Obstet Gynecol. 2020 Nov;136(5):972-980. doi: 10.1097/AOG.0000000000004120. Obstet Gynecol. 2020. PMID: 33030865 Free PMC article.
-
Evidence-based surgical procedures to optimize caesarean outcomes: an overview of systematic reviews.EClinicalMedicine. 2024 May 19;72:102632. doi: 10.1016/j.eclinm.2024.102632. eCollection 2024 Jun. EClinicalMedicine. 2024. PMID: 38812964 Free PMC article. Review.
References
References to studies included in this review
Abdelaziz 2014 {published data only}
-
- Abdelaziz S, Saad H. Opening versus non opening of the cervical canal during caeserian section. Medical Journal of Cairo University 2014;82(2):151‐5.
Ahmed 2005 {published data only}
-
- Ahmed B, Abu Nahia F, Abushama M. Routine cervical dilatation during elective cesarean section and its influence on maternal morbidity: a randomized controlled study. Journal of Perinatal Medicine 2005;33(6):510‐3. - PubMed
Ezegwui 2015 {published data only}
-
- Ezegwui HU, Ogbuefi FC. Routine cervical dilatation during elective caesarean section. Should we continue?. Journal of Obstetrics and Gynaecology 2015;35:150‐2. - PubMed
Güngördük 2009 {published data only}
-
- Gungorduk K, Yildirim G, Ark C. Is routine cervical dilatation necessary during elective caesarean section? A randomised controlled trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 2009;49(3):263‐7. - PubMed
Kirscht 2017 {published data only}
-
- ACTRN12612000228886. Reduction of postoperative morbidity by mechanical dilatation of the cervix at non‐labour caesarean? A randomized controlled trial. anzctr.org.au/Trial/Registration/TrialReview.aspx?id=362136 Date first received: 23 February 2012.
-
- Kirscht J, Weiss C, Nickol J, Berlit S, Tuschy B, Hoch B, et al. Dilatation or no dilatation of the cervix during cesarean section (Dondi Trial): a randomized controlled trial. Archives of Gynecology and Obstetrics 2017;295(1):39‐43. - PubMed
Sakinci 2015 {published data only}
-
- Sakinci M, Kuru O, Olgan S, Gunduz S, Bakir VL, Kaya O, et al. Dilatation of the cervix at non‐labour caesarean section: Does it improve the patients' perception of pain post‐operatively?. Journal of Obstetrics and Gynaecology 2015;35(7):681‐4. - PubMed
Tosun 2011 {published data only}
-
- Tosun M, Sakinci M, Çelik H, Torumtay B, Yazici E, Alper T, et al. A randomized controlled study investigating the necessity of routine cervical dilatation during elective cesarean section. Archives of Gynecology and Obstetrics 2011;284(1):85‐9. - PubMed
-
- Tosun M, Saknc M, Celik H, Torumtay B, Yazc E, Alper T, et al. A randomized controlled study investigating the necessity of routine cervical dilatation during elective cesarean section. Turk Jinekoloji ve Obstetrik Dernegi Dergisi 2010;7(Suppl Kongre Bild):48. - PubMed
Yazicioglu 2012 {published data only}
-
- Yazicioglu HF, Sevket O, Ekin M, Ozyurt O, Aygun M. Incomplete healing of the uterine incision after cesarean section: is it preventable by intraoperative digital dilatation of the internal cervical ostium?. Gynecologic & Obstetric Investigation 2012;74(2):131‐5. - PubMed
References to studies awaiting assessment
Cengiz 2013 {published data only}
-
- NCT01954719. Is routine cervical dilatation necessary during elective caesarean section? a randomised controlled trial. clinicaltrials.gov/ct2/show/record/NCT01954719 (first received: 19 September 2013).
Additional references
Allen 2006
-
- Allen VM, O'Connell CM, Baskett TF. Maternal morbidity associated with cesarean delivery without labor compared with induction of labor at term. Obstetrics & Gynecology 2006;108(2):286‐94. - PubMed
Berlit 2013
-
- Berlit S, Nickol J, Weiss C, Tuschy B, Mayer J, Sütterlin M, et al. Cervical dilatation and curettage in elective caesarean section. a retrospective analysis. In Vivo 2013;26:661‐6. - PubMed
Bollapragada 2002
-
- Bollapragada SS, Edozien LC. Apparent absence of lochia after elective caesarean section. Journal of Obstetrics and Gynaecology 2002;22(5):558. - PubMed
Chanrachakul 2000
-
- Chanrachakul B, Herabutya Y, Udomsubpayakul U. Epidemic of cesarean section at the general, private and university hospitals in Thailand. Journal of Obstetrics and Gynaecology Research 2000;26(5):357‐61. - PubMed
Chanthasenanont 2007
-
- Chanthasenanont A, Pongrojpaw D, Nanthakomon T, Somprasit C, Kamudhamas A, Suwannarurk K. Indications for cesarean section at Thammasart University Hospital. Journal of the Medical Association of Thailand 2007;90:1733‐7. - PubMed
Chongsuvivatwong 2010
-
- Chongsuvivatwong V, Bachtiar H, Chowdhury ME, Fernando S, Suwanrath C, Kor‐Anantakul O, et al. Maternal and fetal mortality and complications associated with cesarean section deliveries in teaching hospitals in Asia. Journal of Obstetrics and Gynaecology Research 2010;36(1):45‐51. - PubMed
GRADEpro GDT [Computer program]
-
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 02/01/17. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015; Vol. Version 3.5.
Higgins 2011
-
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Krebs 2003
-
- Krebs L, Langhoff‐Roos J. Elective cesarean delivery for term breech. Obstetrics & Gynecology 2003;101(4):690‐9. - PubMed
Liu 2007
Lydon‐Rochelle 2006
-
- Lydon‐Rochelle MT, Gardella C, Cardenas V, Easterling TR. Repeat cesarean delivery: what indications are recorded in the medical chart?. Birth 2006;33:4‐11. - PubMed
Magann 2005
-
- Magann EF, Evans S, Hutchinson M, Collins R, Lanneau G, Morrison JC. Postpartum hemorrhage after cesarean delivery: an analysis of risk factors. Southern Medical Journal 2005;98(7):681‐5. - PubMed
Malkamy 1995
-
- Malkamy H, Ardekany MS. Reducing postpartum endometritis by intraoperative cervical dilatation. International Journal of Gynecology & Obstetrics 1995;48(3):325‐6. - PubMed
Myers 2008
-
- Myers KM, Paskaleva AP, House M, Socrate S. Mechanical and biochemical properties of human cervical tissue. Acta Biomaterialia 2008;4(1):104‐16. - PubMed
RevMan 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schünemann 2013
-
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
Sherman 1999
-
- Sherman D, Lurie S, Betzer M, Pinhasi Y, Arieli S, Boldur I. Uterine flora at cesarean and its relationship to postpartum endometritis. Obstetrics & Gynecology 1999;94(5 Pt 1):787‐91. - PubMed
Swende 2007
-
- Swende TZ, Agida ET, Jogo AA. Elective caesarean section at the Federal Medical Centre Makurdi, North Central Nigeria. Nigerian Journal of Medicine 2007;16(4):372‐4. - PubMed
Van der Walt 1994
-
- Walt WA, Cronje HS, Bam RH. Vaginal delivery after one cesarean section. International Journal of Gynecology & Obstetrics 1994;46(3):271‐7. - PubMed
Van Roosmalen 1995
-
- Roosmalen J, Does CD. Caesarean birth rates worldwide. A search for determinants. Tropical and Geographical Medicine 1995;47(1):19‐22. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical