

Management of Small Bowel Neuroendocrine Tumors
- PMID: 30096273
- PMCID: PMC6091496
- DOI: 10.1200/JOP.18.00135
Management of Small Bowel Neuroendocrine Tumors
Abstract
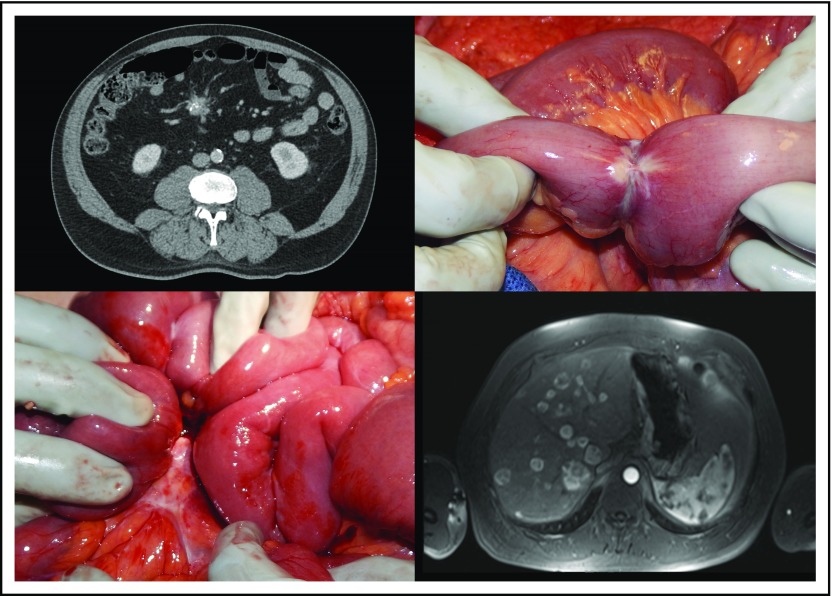
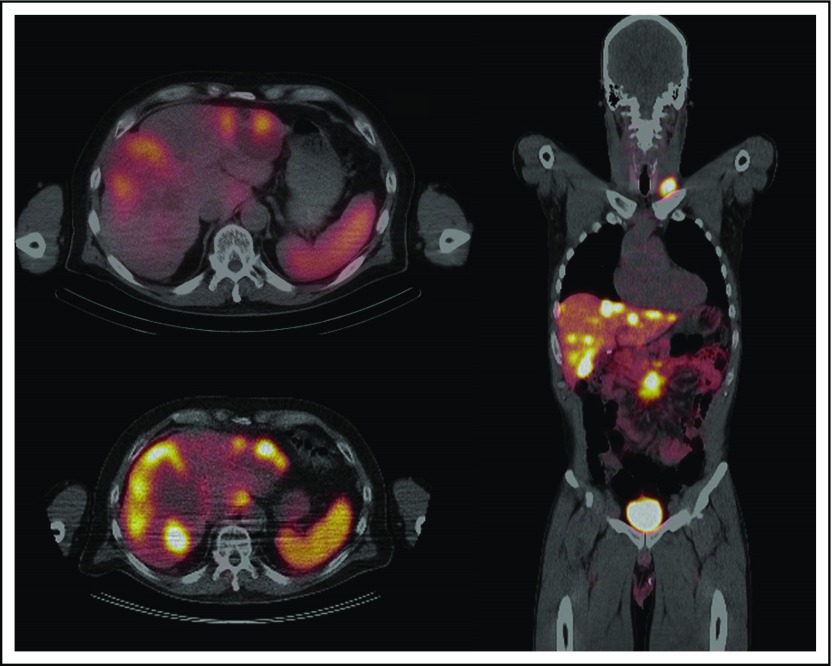
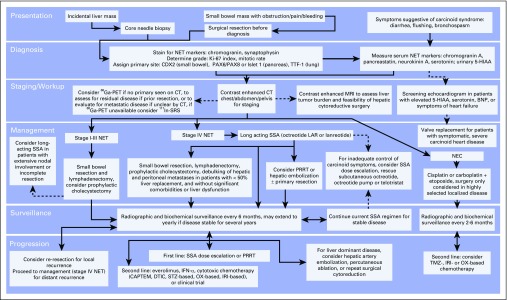
Small bowel neuroendocrine tumors (NETs) are increasing in incidence and are now the most common primary malignancies of the small intestine. Despite this increase, the vague presentation and slow growth of these tumors lead to long delays in diagnosis, and many patients present with metastases. Patients with metastatic small bowel NETs have a favorable disease prognosis, particularly when contrasted with other GI malignancies, and benefit from aggressive, multimodal therapy. During the past decade, the options for the diagnosis and treatment of small bowel NETs have increased considerably. This review provides a practical framework for the physician who seek to understand the epidemiology, presentation, diagnosis, and management of small bowel NETs.
Figures
Comment in
-
Progress in the Evaluation and Treatment of Small Bowel Neuroendocrine Tumors.J Oncol Pract. 2018 Aug;14(8):487-489. doi: 10.1200/JOP.18.00440. J Oncol Pract. 2018. PMID: 30096272 No abstract available.
-
Small Bowel Neuroendocrine Tumors: Big Advances in the Land of Small Tumors.J Oncol Pract. 2018 Aug;14(8):485-486. doi: 10.1200/JOP.18.00392. J Oncol Pract. 2018. PMID: 30096275 No abstract available.
References
-
- Langhans T. Ueber einen drüsenpolyp im ileum. Virchows Arch. 1867;38:559–560.
-
- Lubarsch O. Ueber den primären krebs des ileum nebst bemerkungen über das gleichzeitige vorkommen von krebs und tuberculose. Virchows Arch. 1888;111:280–317.
-
- Ransom WB. A case of primary carcinoma of the ileum. Lancet. 1890;136:1020–1023.
-
- Oberndorfer S. Karzinoide tumoren des dünndarms. Frankf Z Pathol. 1907;1:425–432.
-
- Williams ED, Sandler M. The classification of carcinoid tumours. Lancet. 1963;1:238–239. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
