

Double-blind, randomized, multicenter phase 2 study of SC411 in children with sickle cell disease (SCOT trial)
- PMID: 30097463
- PMCID: PMC6093734
- DOI: 10.1182/bloodadvances.2018021444
Double-blind, randomized, multicenter phase 2 study of SC411 in children with sickle cell disease (SCOT trial)
Abstract
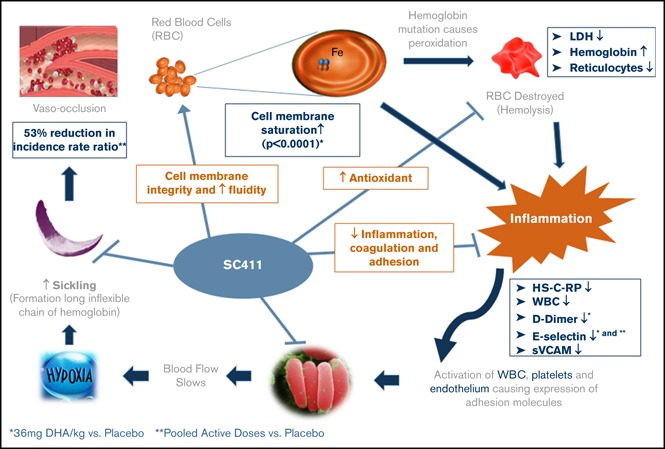
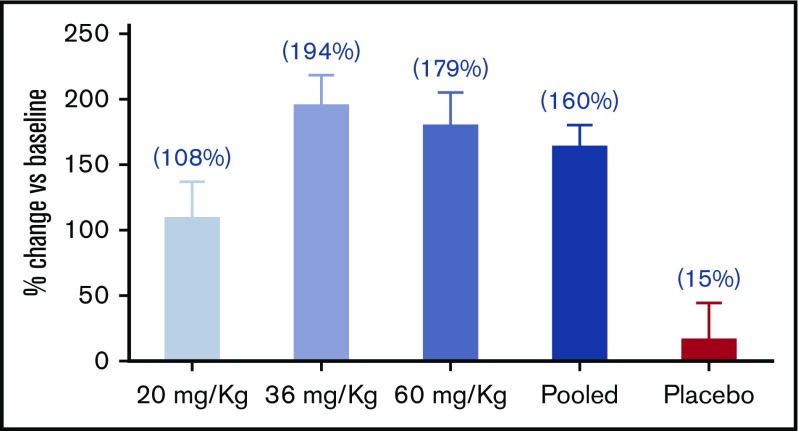
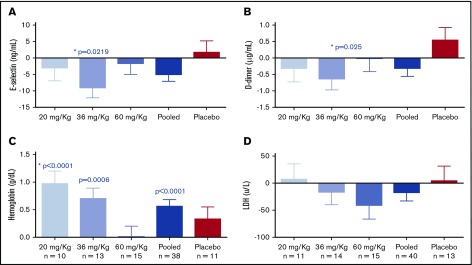
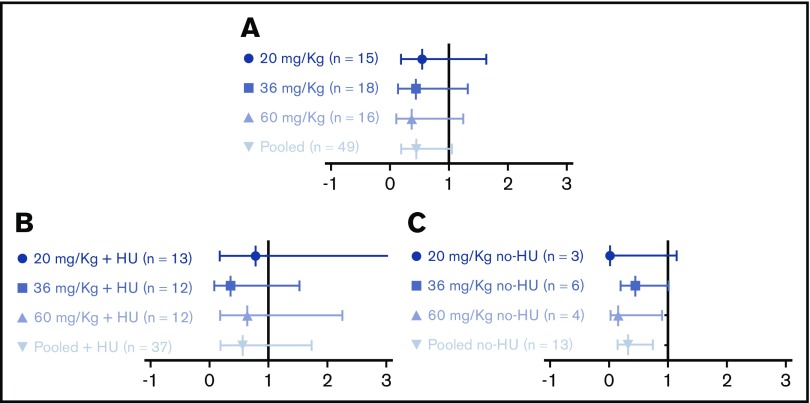
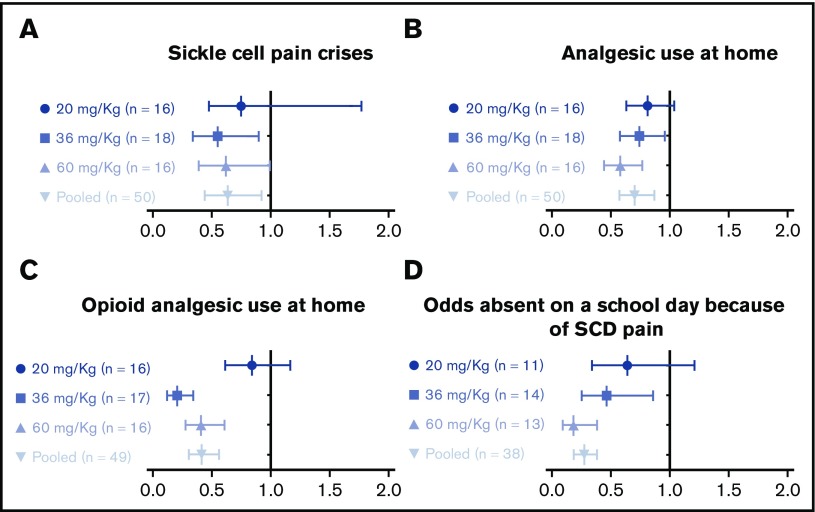
Blood cell membranes in sickle cell disease (SCD) have low docosahexaenoic acid (DHA). DHA treatment reduces sickle cell crisis (SCC) rate and ameliorates the inflammation, oxidative stress, and hypercoagulable state of SCD. SC411 is a novel DHA ethyl ester formulation with a proprietary delivery platform (Advanced Lipid Technology) that enhances DHA bioavailability. The SCOT trial investigated the effect of 3 different doses of SC411 on clinical and biochemical endpoints in 67 children with SCD (5-17 years old). Seventy-six percent of subjects were also receiving hydroxyurea. After 4 weeks of treatment with SC411 at 20, 36, and 60 mg DHA/kg per day or placebo a statistically significant (P < .001) mean percentage increase of blood cell membrane DHA and eicosapentaenoic acid was seen vs baseline: 109.0% (confidence interval [CI], 46.7-171.3), 163.8% (CI, 108.3-219.2), 170.8% (CI, 90.2-251.4), and 28.6% (CI, 250.1 to 107.3), respectively. After 8 weeks of treatment, statistically significant changes vs placebo were also observed in D-dimer (P = .025) and soluble E-selectin (P = .0219) in subjects exposed to 36 mg/kg. A significant increase in hemoglobin was observed against placebo in subjects receiving 20 mg DHA/kg per day (P = .039). SC411 significantly reduced electronic diary recorded SCC, analgesic use at home, and days absent from school because of sickle cell pain. The lower rate of clinical SCC observed in the pooled active groups vs placebo did not reach statistical significance (rate ratio, 0.47; 95% CI, 0.20-1.11; P = .07). All tested doses were safe and well tolerated. This trial was registered at www.clinicaltrials.gov as #NCT02973360.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: A.A.D. and A.L.R. are employees of SCI. O.A.A. has been an advisory board member for Novartis. C.D.D. has been an advisory board member for Novartis, Pfizer, and SCI; worked as a consultant for Novartis, Pfizer, GBT, Epizyme, and Prolong Therapeutics, and Data and Safety Monitoring Committee chair for Ironwood; and obtained research funding for Pfizer, SCI, Lilly, Novartis, Katz Foundation, and the National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health and Human Development. J.K. has worked as a consultant for Bluebird Bio, Novartis, CRISPR, and AstraZeneca (steering committee), as well as participated in the National Heart, Lung, and Blood Institute Sickle Cell Advisory Committee. L.V.B. has worked as a consultant for Prolong Pharmaceuticals and Mast Therapeutics; been a paid member of the American Society of Pediatric Hematology/Oncology; participated in the advisory committee of Bioverativ; and obtained research funding from the National Institutes of Health, Pfizer, and Mast Therapeutics. M.U.C. participated in the Advisory Board of Shire, Octapharma, Grifols, Pfizer, Bayer, Roche, Bioverativ, and Hema; has been part of the Speakers Bureau of Shire, Roche/Genentech, Bayer, and Novo Nordisk; has obtained research support from Shire and Pfizer; has participated as site investigator for Pfizer, Roche/Genentech, Novo Nordisk, Global Blood Therapeutics, SCI, and Amgen; and holds stocks in Alnylum Pharmaceuticals. L.N. worked as a consultant for Emmaus, Bayer, CTD Holdings, and Pfizer; is currently on a Data and Safety Monitoring Committee for ApoPharma; is a site principal investigator for Pfizer, Sancilio, and PCORI; is a co-investigator for ApoPharma, Novartis, Bluebird Bio, Sangamo Therapeutics, Global Blood Therapeutics, Silarus, Celgene, Terumo, La Jolla Pharmaceuticals, and Imara; and also is an investigator on National Heart, Lung, and Blood Institute, Agency for Healthcare Research and Quality, US Food and Drug Administration, Health Resources and Services Administration, Centers for Disease Control and Prevention, Doris Duke, the State of California, University of California Office of the President, and Seattle Children's Research grants. F.S. has worked as a consultant for Clearway Global, LLC; and is a member of the Board of Directors of SCI; and participated in the Advisory Committees of Noble Financial Company. M.M.H. has worked as a consultant for SCI and AstraZeneca; is part of the Advisory Committees of SCI and Novartis; and received research support from SCI, Pfizer, and Intrinsic Life Sciences. The remaining authors declare no competing financial interests.
Figures

References
-
- Piel FB, Steinberg MH, Rees DC. Sickle cell disease. N Engl J Med. 2017;376(16):1561-1573. - PubMed
-
- Hassell KL. Population estimates of sickle cell disease in the U.S. Am J Prev Med. 2010;38(4 Suppl):S512-S521. - PubMed
-
- Rahimy MC, Gangbo A, Ahouignan G, et al. . Effect of a comprehensive clinical care program on disease course in severely ill children with sickle cell anemia in a sub-Saharan African setting. Blood. 2003;102(3):834-838. - PubMed
-
- Molineaux L, Fleming AF, Cornille-Brøgger R, Kagan I, Storey J. Abnormal haemoglobins in the Sudan savanna of Nigeria. III. Malaria, immunoglobulins and antimalarial antibodies in sickle cell disease. Ann Trop Med Parasitol. 1979;73(4):301-310. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
