

Optimizing Cancer Treatment Using Game Theory: A Review
- PMID: 30098166
- PMCID: PMC6947530
- DOI: 10.1001/jamaoncol.2018.3395
Optimizing Cancer Treatment Using Game Theory: A Review
Abstract
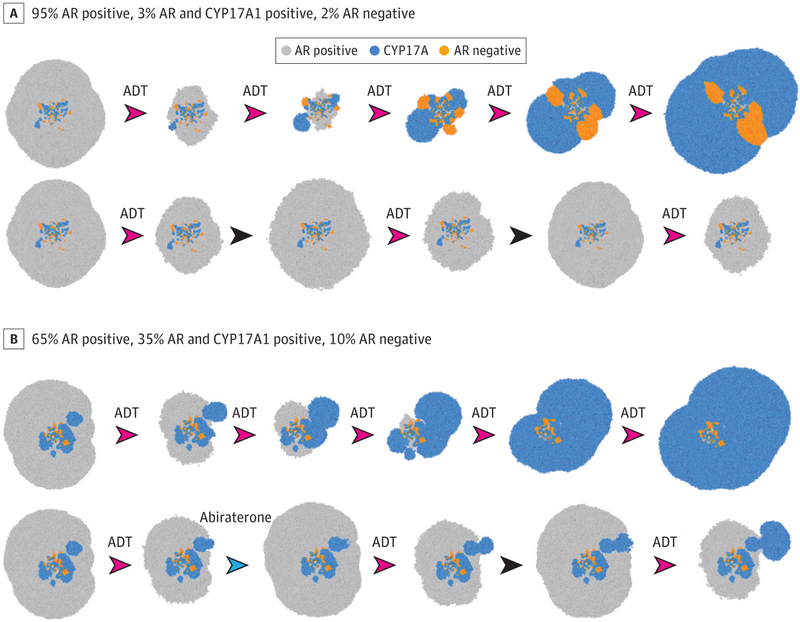
Importance: While systemic therapy for disseminated cancer is often initially successful, malignant cells, using diverse adaptive strategies encoded in the human genome, almost invariably evolve resistance, leading to treatment failure. Thus, the Darwinian dynamics of resistance are formidable barriers to all forms of systemic cancer treatment but rarely integrated into clinical trial design or included within precision oncology initiatives.
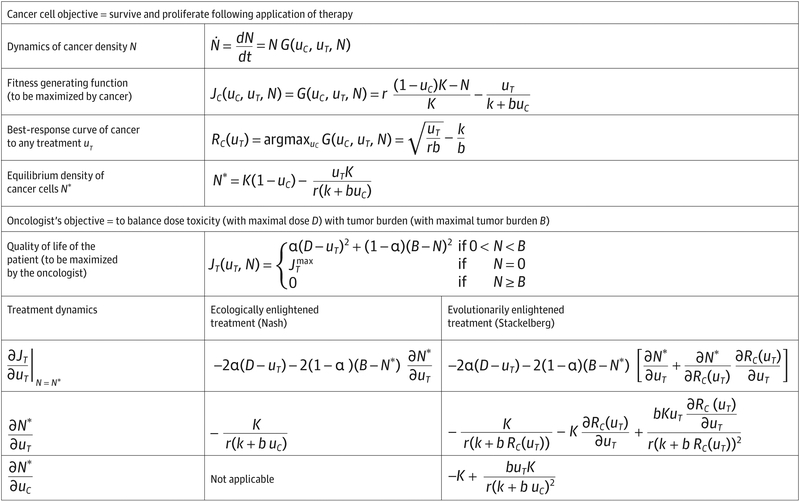
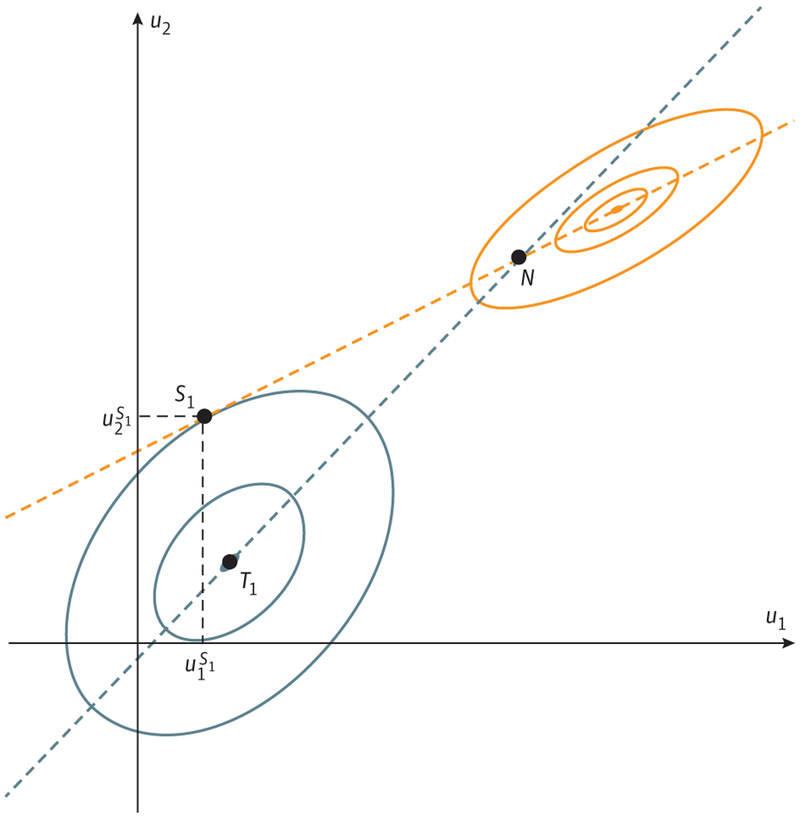
Observations: We investigate cancer treatment as a game theoretic contest between the physician's therapy and the cancer cells' resistance strategies. This game has 2 critical asymmetries: (1) Only the physician can play rationally. Cancer cells, like all evolving organisms, can only adapt to current conditions; they can neither anticipate nor evolve adaptations for treatments that the physician has not yet applied. (2) It has a distinctive leader-follower (or "Stackelberg") dynamics; the "leader" oncologist plays first and the "follower" cancer cells then respond and adapt to therapy. Current treatment protocols for metastatic cancer typically exploit neither asymmetry. By repeatedly administering the same drug(s) until disease progression, the physician "plays" a fixed strategy even as the opposing cancer cells continuously evolve successful adaptive responses. Furthermore, by changing treatment only when the tumor progresses, the physician cedes leadership to the cancer cells and treatment failure becomes nearly inevitable. Without fundamental changes in strategy, standard-of-care cancer therapy typically results in "Nash solutions" in which no unilateral change in treatment can favorably alter the outcome.
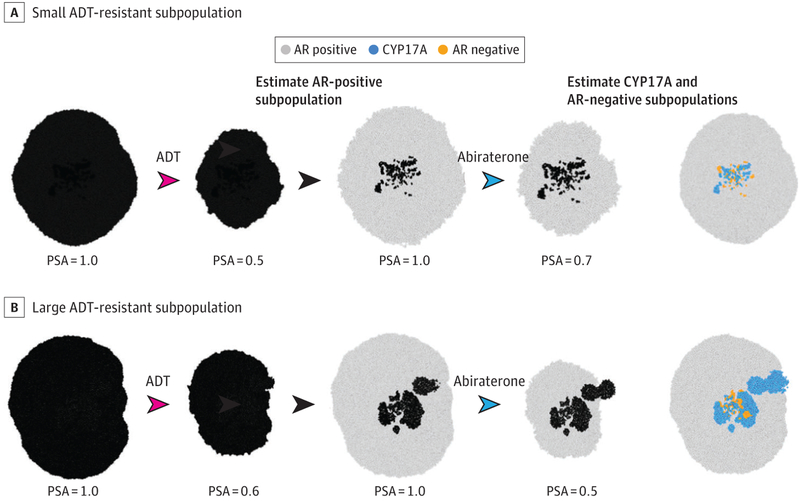
Conclusions and relevance: Physicians can exploit the advantages inherent in the asymmetries of the cancer treatment game, and likely improve outcomes, by adopting more dynamic treatment protocols that integrate eco-evolutionary dynamics and modulate therapy accordingly. Implementing this approach will require new metrics of tumor response that incorporate both ecological (ie, size) and evolutionary (ie, molecular mechanisms of resistance and relative size of resistant population) changes.
Conflict of interest statement
Figures
References
-
- Von Neumann J, Morgenstern O. Theory of Games and Economic Behavior. 3rd ed Princeton, NJ: Princeton University Press; 1953.
-
- Myerson RB. Game Theory: Analysis of Conflict. Cambridge, MA: Harvard University Press; 1991.
-
- Aumann RJ, Hart S, Young HP, Zamir S. Handbook of Game Theory With Economic Applications. New York, NY: Elsevier; 1992.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
