

Atraumatic Scala Tympani Cochleostomy; Resolution of the Dilemma
- PMID: 30100542
- PMCID: PMC6354452
- DOI: 10.5152/iao.2018.4974
Atraumatic Scala Tympani Cochleostomy; Resolution of the Dilemma
Abstract
Objectives: While an accurate placement in cochleostomy is critical to ensure appropriate insertion of the cochlear implant (CI) electrode into the scala tympani (ST), the choice of preferred cochleostomy sites widely varied among experienced surgeons. We present a novel technique for precise yet readily applicable localization of the optimum site for performing ST cochleostomy.
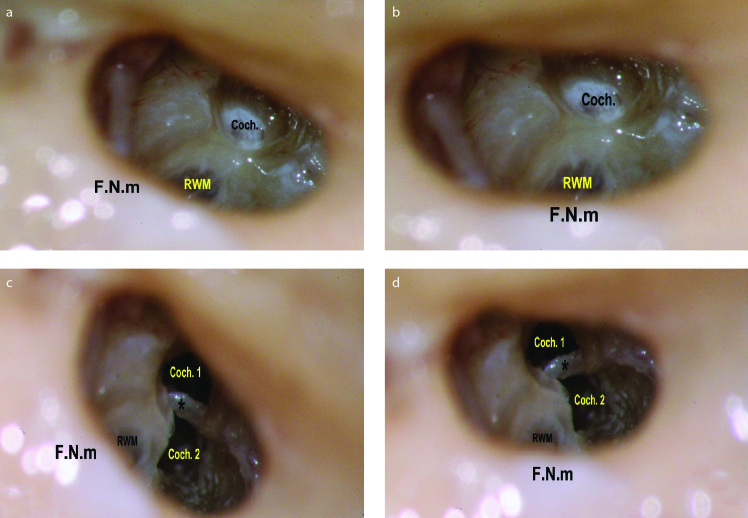
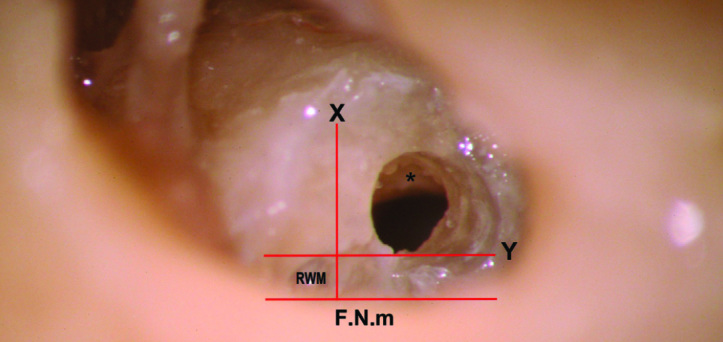
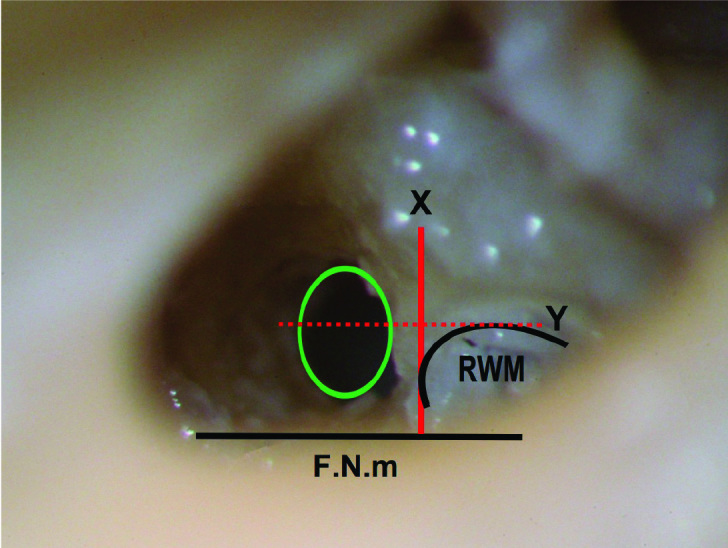
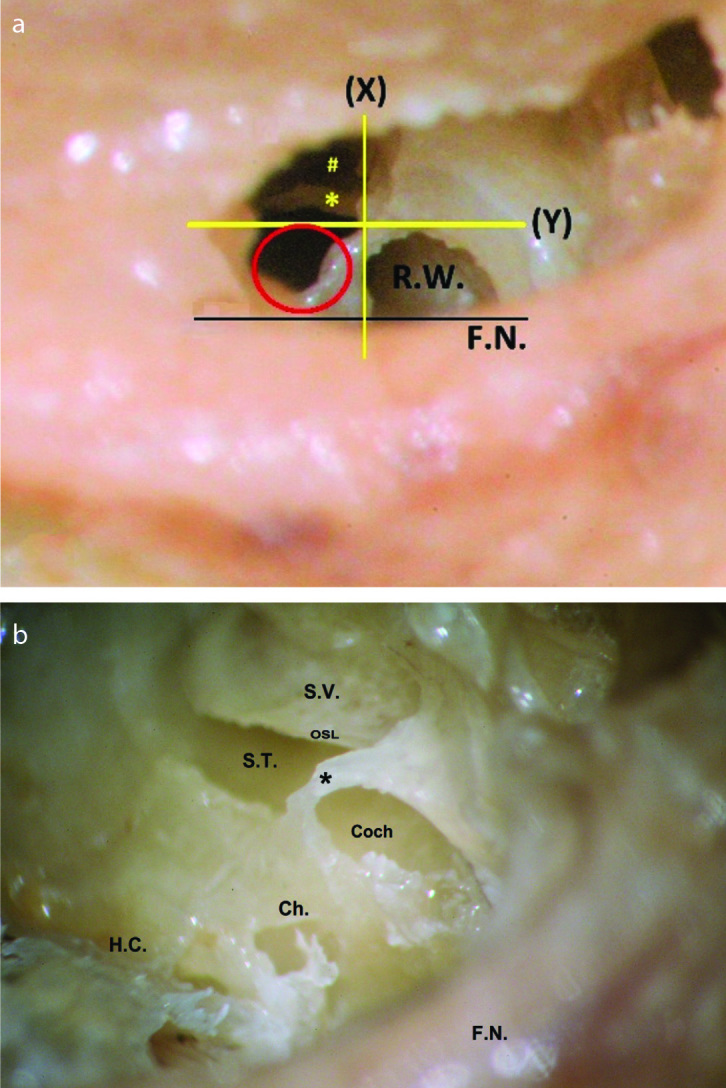
Material and methods: Twenty fresh frozen temporal bones were dissected using the mastoidectomy-posterior tympanotomy approach. Based on the facial nerve and the margins of the round window membrane (RWM), the cochleostomy site was chosen to insert the electrode into the ST while preserving the surrounding intracochlear structures.
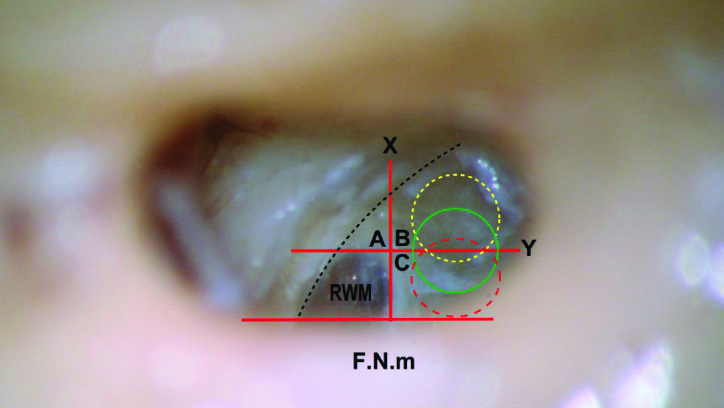
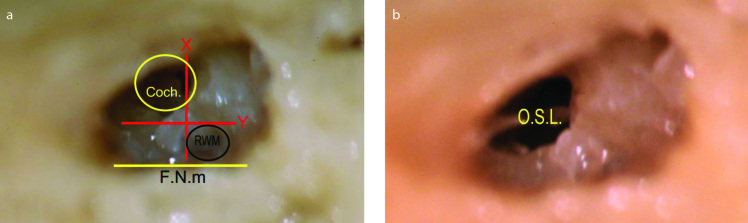
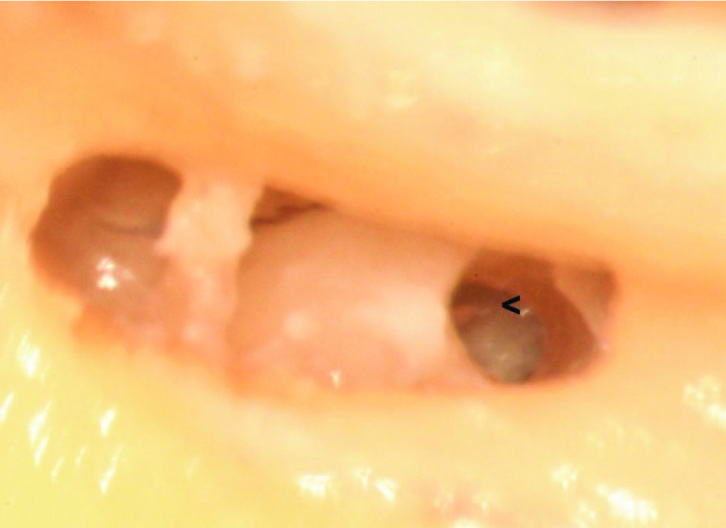
Results: There is a limited safe area suitable for the ST implantation in the area inferior and anterior to the RWM. There is a higher risk of scala vestibuli (SV) insertion anterior to that area. Posterior to that area, the cochlear aqueduct (CA) and inferior cochlear vein (ICV) are liable for the injury.
Conclusion: For atraumatic CI, precise and easy localization of the site of cochleostomy play a pivotal role in preserving intracochlear structures. Accurate setting of the vertical and horizontal orientations is mandatory before choosing the site of cochleostomy. The facial nerve and the margins of the RWM offer a very helpful clue for such localization; meanwhile, it is readily identifiable in the surgical field.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
