

Cost-minimization analysis of degludec/liraglutide versus glargine/aspart: economic implications of the DUAL VII study outcomes
- PMID: 30100746
- PMCID: PMC6067612
- DOI: 10.2147/CEOR.S169045
Cost-minimization analysis of degludec/liraglutide versus glargine/aspart: economic implications of the DUAL VII study outcomes
Abstract
Background: Diabetes represents a relevant public health problem worldwide due to its increasing prevalence and socioeconomic burden. There is no doubt that tight glycemic control reduces the development of diabetic complications such as the long-term costs related to the disease. The aim of our model was to calculate total direct costs associated with the two treatments considered in DUAL VII study, and hence evaluate the potential economic benefits for the National Health System (NHS) deriving from the use of insulin degludec plus liraglutide (IDegLira) in a once-daily fixed combination.
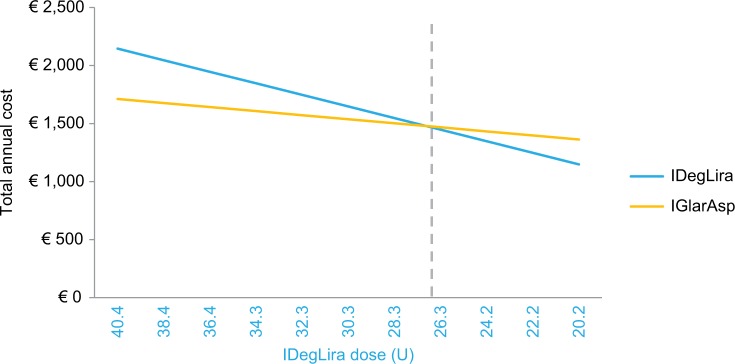
Materials and methods: We applied the cost-minimization technique adopting the NHS point of view to the DUAL VII trial outcomes. In the model, developed in Microsoft Excel®, we calculated and compared annual costs per patient of the two therapeutic options for type 2 diabetes (T2D) patients not achieving glycemic control on basal insulin and metformin described in the trial, including costs of therapy management and side effects, both negative and positive. Annual treatment costs were calculated based on IDegLira and basal bolus end-of-trial doses resulting in a 1:2 ratio (40.4 U vs 84.1 U). Therefore, maintaining the IDegLira/basal bolus at 1:2 dose ratio, we calculated the correlation between the dose reduction and costs compared to DUAL VII doses base case scenario.
Results: Total treatment costs were obtained by adding annual cost of drug, needles, glycemic self-monitoring, hypoglycemic events, and effect on consumption of other drugs. Total annual costs of IDegLira combination resulted in €434 higher than basal bolus in DUAL VII base case (40.4 U); the two treatments reported equal costs at 34% dose reduction (26.7 U), while below this value IDegLira treatment became less expensive, with about €215 gain at 50% dose reduction (20.2 U). It is also important to notice that above the break-even point, until an IDegLira dose of 30 U, the cost difference is negligible in view of the clinical benefit provided by the fixed combination highlighted in DUAL VII trial.
Conclusion: Adding the significant clinical findings derived from DUAL VII trial to our economic evaluation, IDegLira seems to offer an important alternative to basal-bolus therapy.
Keywords: IDegLira; basal-bolus therapy; cost minimization; diabetes.
Conflict of interest statement
Disclosure ET has received consultancy and/or speaking fees and research grants from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Johnson & Johnson, MSD Italy, Novo Nordisk, Sanofi, and Takeda, over the last 3 years. GLC received research and educational grants from Abbott, Amgen, DOC Generici, Eisai, LeoPharma, Menarini, Merck Sharp and Dohme, Novo Nordisk, Sanofi, and Takeda. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Evaluation of the Short-Term Cost-Effectiveness of IDegLira Versus Basal Insulin and Basal-Bolus Therapy in Patients with Type 2 Diabetes Based on Attainment of Clinically Relevant Treatment Targets.J Manag Care Spec Pharm. 2020 Feb;26(2):143-153. doi: 10.18553/jmcp.2019.19035. Epub 2019 Dec 19. J Manag Care Spec Pharm. 2020. PMID: 31856636 Free PMC article. Clinical Trial.
-
Ideglira is Associated With Improved Short-Term Clinical Outcomes and Cost Savings Compared with Insulin Glargine U100 Plus Insulin Aspart in the U.S.Endocr Pract. 2018 Sep;24(9):796-804. doi: 10.4158/EP-2018-0134. Endocr Pract. 2018. PMID: 30308134
-
The management of type 2 diabetes with fixed-ratio combination insulin degludec/liraglutide (IDegLira) versus basal-bolus therapy (insulin glargine U100 plus insulin aspart): A short-term cost-effectiveness analysis in the UK setting.Diabetes Obes Metab. 2018 Oct;20(10):2371-2378. doi: 10.1111/dom.13375. Epub 2018 Jun 25. Diabetes Obes Metab. 2018. PMID: 29797389 Free PMC article.
-
Pharmacoeconomic Review Report: Insulin degludec and liraglutide injection (Xultophy): (Novo Nordisk Canada Inc.): Indication: An adjunct to lifestyle modifications, for the once-daily treatment of adults with type 2 diabetes mellitus to improve glycemic control in combination with metformin, with or without sulfonylurea, when these combined with basal insulin (less than 50 U daily) or liraglutide (less than or equal to 1.8 mg daily) do not provide adequate glycemic control [Internet].Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2019 Dec. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2019 Dec. PMID: 32182000 Free Books & Documents. Review.
-
Clinical Considerations When Initiating and Titrating Insulin Degludec/Liraglutide (IDegLira) in People with Type 2 Diabetes.Drugs. 2020 Feb;80(2):147-165. doi: 10.1007/s40265-019-01245-3. Drugs. 2020. PMID: 31960258 Free PMC article. Review.
Cited by
-
Cost-Utility Analysis of Saxagliptin/Dapagliflozin Versus Gliclazide and Insulin Glargine: Economic Implications of the Outcomes of the CVD-Real Studies I and II.Health Serv Insights. 2020 Jun 16;13:1178632920929982. doi: 10.1177/1178632920929982. eCollection 2020. Health Serv Insights. 2020. PMID: 32595277 Free PMC article.
-
Delphi-Based Consensus on Treatment Intensification in Type 2 Diabetes Subjects Failing Basal Insulin Supported Oral Treatment: Focus on Basal Insulin + GLP-1 Receptor Agonist Combination Therapies.Diabetes Ther. 2021 Mar;12(3):781-800. doi: 10.1007/s13300-021-01012-2. Epub 2021 Feb 7. Diabetes Ther. 2021. PMID: 33550569 Free PMC article.
-
Value For Money In The Treatment Of Patients With Type 2 Diabetes Mellitus: Assessing The Long-Term Cost-Effectiveness Of IDegLira Versus iGlarLixi In Italy.Clinicoecon Outcomes Res. 2019 Oct 7;11:605-614. doi: 10.2147/CEOR.S218746. eCollection 2019. Clinicoecon Outcomes Res. 2019. PMID: 31632108 Free PMC article.
-
Pharmacoeconomic Aspects of Diabetes Mellitus: Outcomes and Analysis of Health Benefits Approach.Curr Diabetes Rev. 2024;20(8):12-22. doi: 10.2174/0115733998246567230924134603. Curr Diabetes Rev. 2024. PMID: 37842896 Review.
-
Association of glycosylated hemoglobin and outcomes in patients with COVID-19 and pre-existing type 2 diabetes: A protocol for systematic review and meta-analysis.Medicine (Baltimore). 2020 Nov 20;99(47):e23392. doi: 10.1097/MD.0000000000023392. Medicine (Baltimore). 2020. PMID: 33217883 Free PMC article.
References
-
- ISTAT 2017 [National Institute of Statistics] Diabetes in Italy Years 2000–2016. [Accessed January 30, 2018]. Available from: https://www.istat.it/en/files/2017/07/Report_Diabetes_En_def.pdf?title=D....
-
- UK Prospective Diabetes Study (UKPDS) Group Intensive blood glucose control with sulphonilureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–853. - PubMed
-
- The Diabetes Control and Complications Trial Research Group The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–986. - PubMed
-
- Cryer PE. Hypoglycemia is the limiting factor in the management of diabetes. Diabetes Metab Res Rev. 1999;15:42–46. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
