

Diagnosis, Pathological Findings, and Clinical Management of Gangliocytic Paraganglioma: A Systematic Review
- PMID: 30101131
- PMCID: PMC6072869
- DOI: 10.3389/fonc.2018.00291
Diagnosis, Pathological Findings, and Clinical Management of Gangliocytic Paraganglioma: A Systematic Review
Abstract
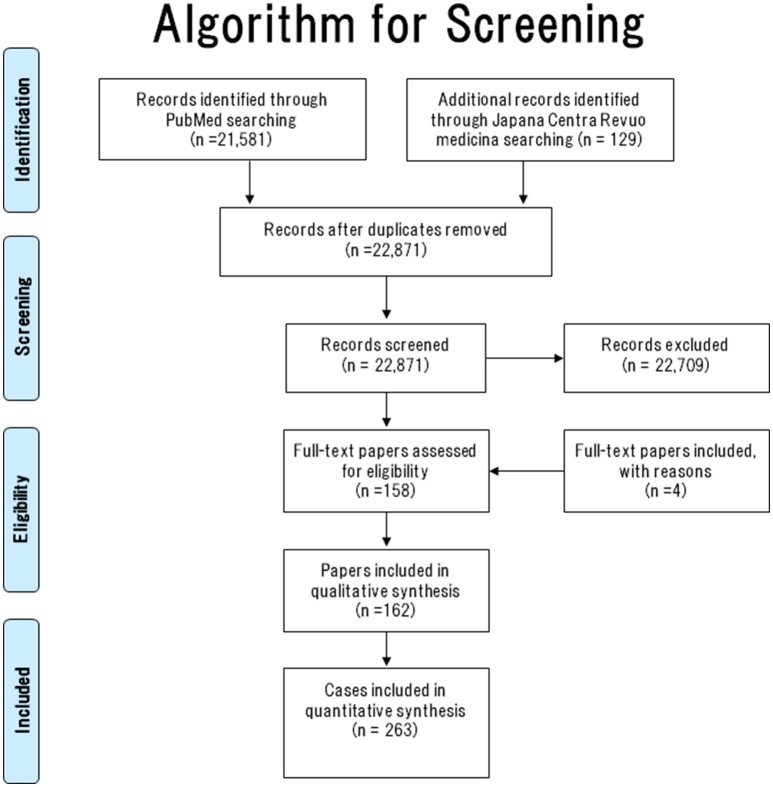
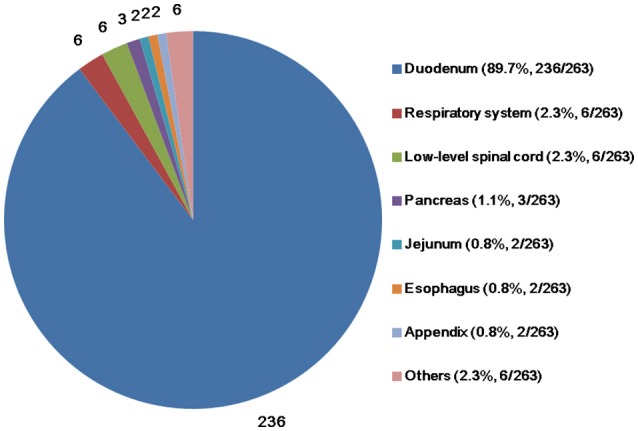
Background: Although gangliocytic paraganglioma (GP) is considered a rare benign neuroendocrine tumor, cases of mortality have been reported. Occasionally, GP is misdiagnosed as neuroendocrine tumor G1, which is associated with a poorer prognosis than GP. To avoid such misdiagnoses, it is important to understand the clinicopathological characteristics of GP. Thus, herein, we discuss the current literature on the clinicopathological characteristics of GP. Methods: We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. PubMed and Japana Centra Revuo Medicina searches were used to identify papers describing GP. Inclusion criteria included confirmation of epithelioid, spindle-shaped, and ganglion-like cells in the main article and/or figures and whether the paper was cited in other studies of GP. Data were collected on age, sex, site of the primary lesion, tumor size, treatment, prognosis, lymph node metastasis (LNM), depth of tumor invasion, rate of preoperative diagnosis, and clinical symptoms. Results: In total, 162 papers containing 263 cases of GP met the criteria. The mean age at diagnosis was 53.5 years. The male-to-female ratio was 157:104. The mean tumor size was 25.7 mm. The predominant site of the primary tumor was the duodenum (89.7%). The most common clinical sign of GP was gastrointestinal bleeding (47.9%). Other signs and symptoms of GP included abdominal pain (44.7%), anemia (20.3%), incidental findings (12.9%), nausea (6.9%), weight loss (5.5%), general fatigue (5.1%), jaundice (4.6%), and incidental autopsy findings (5.1%). LNM was observed in 11.4% of patients. Liver metastasis was observed in 1.1% of patients. Depth of tumor invasion (penetrating beyond the submucosal layer or sphincter of Oddi) was by far the most significant risk factor for LNM in patients with GP. This suggests, along with histological heterogeneity, that GP may have hamartomatous characteristics. Furthermore, immunohistochemical expression of progesterone receptor and pancreatic polypeptide were useful in distinguishing between GP and neuroendocrine tumor G1, even in small biopsy specimens. Conclusions: We reveal the clinicopathological characteristics of GP, including risk factors for LNM, differential diagnostic approaches, and improvements in the clinical management of this tumor.In addition, GP may have hamartomatous characteristics.
Keywords: gangliocytic paraganglioma; literature survey; metastasis; neuroendocrine tumor; pancreatic polypeptide; progesterone receptor.
Figures
References
-
- Amin SM, Albrechtsen NW, Forster J, Damjanov I. Gangliocytic paraganglioma of duodenum metastatic to lymph nodes and liver and extending into the retropancreatic space. Pathologica (2013) 105:90–3. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous