

Incidence, prevalence, mortality and chronic renal damage of anti-neutrophil cytoplasmic antibody-associated glomerulonephritis in a 20-year population-based cohort
- PMID: 30102330
- PMCID: PMC6735586
- DOI: 10.1093/ndt/gfy250
Incidence, prevalence, mortality and chronic renal damage of anti-neutrophil cytoplasmic antibody-associated glomerulonephritis in a 20-year population-based cohort
Abstract
Background: True population-based clinical and outcomes data are lacking for anti-neutrophil cytoplasmic autoantibody (ANCA)-associated glomerulonephritis (AAGN). Therefore we aimed to estimate the incidence, prevalence and mortality of AAGN, as well as the relationship between the grade of chronic renal damage at presentation and renal and non-renal outcomes.
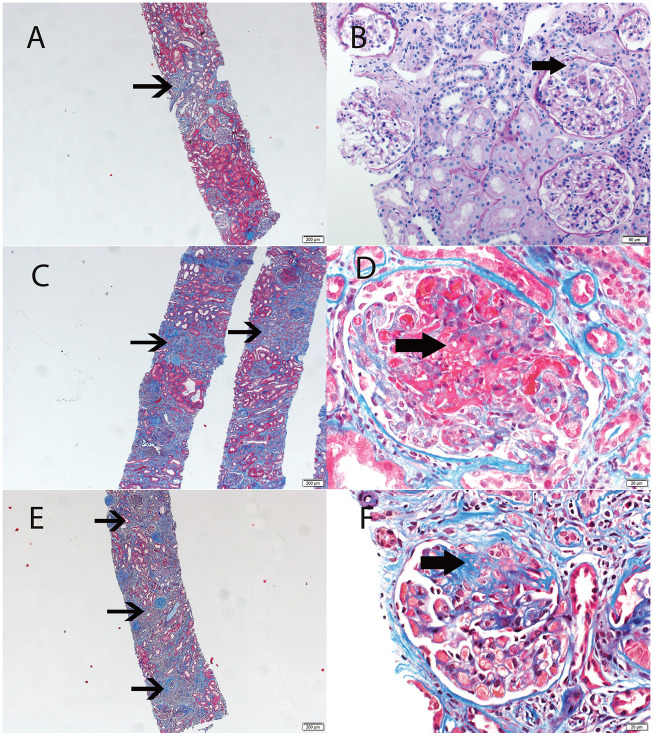
Methods: Patients with AAGN were identified among a population-based incident cohort of 57 Olmsted County residents diagnosed with ANCA-associated vasculitis (AAV) in 1996-2015. Incidence rates were age and sex adjusted to the 2010 US white population. Age- and sex-adjusted prevalence was calculated for 1 January 2015. Survival rates were compared with expected rates in the Minnesota population. Chronic renal damage was assessed by chronicity score (CS) on biopsies performed at diagnosis.
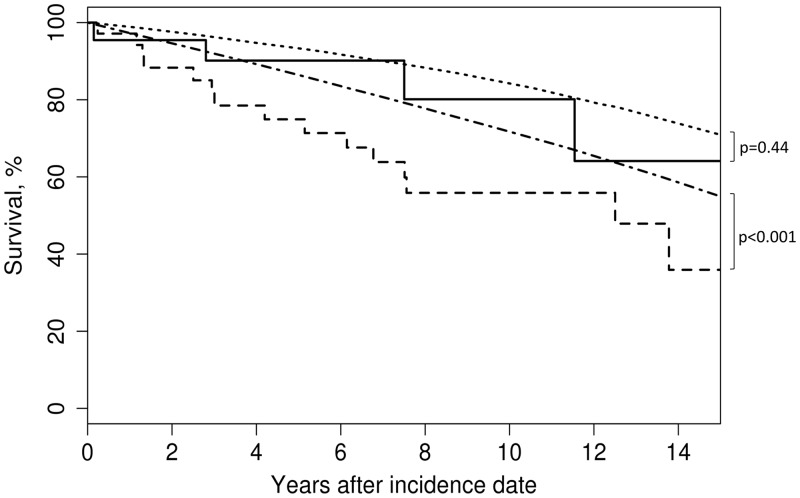
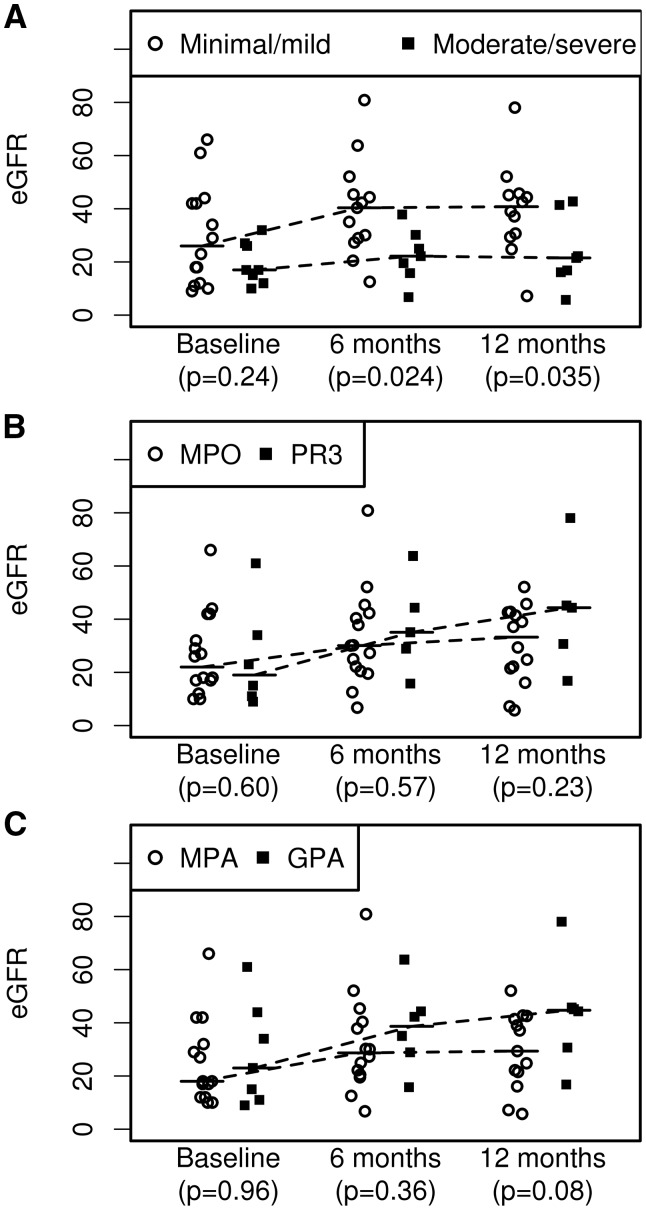
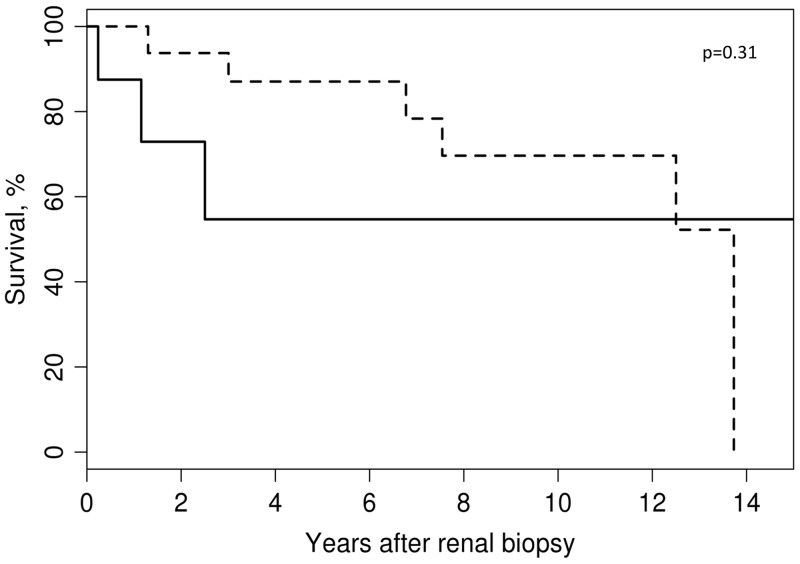
Results: Thirty-four (60%) patients had AAGN. Of these, 65% had microscopic polyangiitis (MPA) and 74% were myeloperoxidase (MPO)-ANCA positive. The annual incidence of AAGN was 2.0/100 000 population [95% confidence interval (CI) 1.3-2.7] and the overall prevalence was 35/100 000 (95% CI 24-47). Mortality for AAGN was increased (P < 0.001), whereas mortality for AAV without glomerulonephritis did not differ from the general population. Minimal to mild CS predicted recovery of renal function at 1 year; clinical diagnosis (granulomatosis with polyangiitis versus MPA) and ANCA specificity (proteinase 3 versus MPO) did not. This observation was replicated in an independent cohort of 38 newly diagnosed AAGN patients seen at our centre over the 1999-2014 period.
Conclusions: The annual incidence and prevalence of AAGN in Minnesota are 2.0/100 000 and 35/100 000, respectively. Mortality is worse compared with AAV patients without glomerulonephritis. More advanced renal damage at diagnosis predicts less renal recovery.
Keywords: ANCA-associated vasculitis; glomerulonephritis; granulomatosis with polyangiitis; nephritis; renal insufficiency.
© The Author(s) 2018. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Figures
Comment in
-
Estimating the epidemiology of anti-neutrophil cytoplasm antibody-associated renal vasculitis and the role of histologic chronicity in predicting renal outcomes.Nephrol Dial Transplant. 2019 Sep 1;34(9):1429-1432. doi: 10.1093/ndt/gfy402. Nephrol Dial Transplant. 2019. PMID: 30649435 No abstract available.
References
-
- Sinico RA, Di Toma L, Radice A.. Renal involvement in anti-neutrophil cytoplasmic autoantibody associated vasculitis. Autoimmun Rev 2013; 12: 477–482 - PubMed
-
- Cornec D, Cornec-Le Gall E, Specks U.. Clinical trials in antineutrophil cytoplasmic antibody-associated vasculitis: what we have learnt so far, and what we still have to learn. Nephrol Dial Transplant 2017; 32(Suppl 1): i37–i47 - PubMed
-
- Mohammad AJ, Jacobsson LT, Westman KW. et al. Incidence and survival rates in Wegener’s granulomatosis, microscopic polyangiitis, Churg-Strauss syndrome and polyarteritis nodosa. Rheumatology (Oxford) 2009; 48: 1560–1565 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
