

Recrudescence, Reinfection, or Relapse? A More Rigorous Framework to Assess Chloroquine Efficacy for Plasmodium vivax Malaria
- PMID: 30102351
- PMCID: PMC6306015
- DOI: 10.1093/infdis/jiy484
Recrudescence, Reinfection, or Relapse? A More Rigorous Framework to Assess Chloroquine Efficacy for Plasmodium vivax Malaria
Abstract
Background: Plasmodium vivax resistance to chloroquine (CQ) has been reported worldwide, although the World Health Organization clinical drug efficacy studies protocol does not permit classification of patient outcomes.
Methods: We enrolled 40 patients with P. vivax malaria in northeastern Cambodia, where >17% treatment failures were previously reported. Patients were treated with CQ (30 mg/kg) and followed for 2 months, with frequent clinical examination and capillary blood sample collection for microscopy, molecular parasite detection and genotyping, and drug concentration measurements. Reinfections were prevented by relocating patients to a transmission-free area.
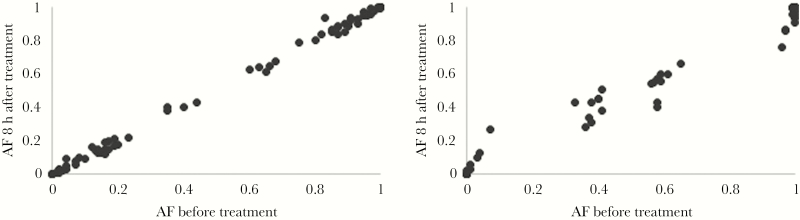
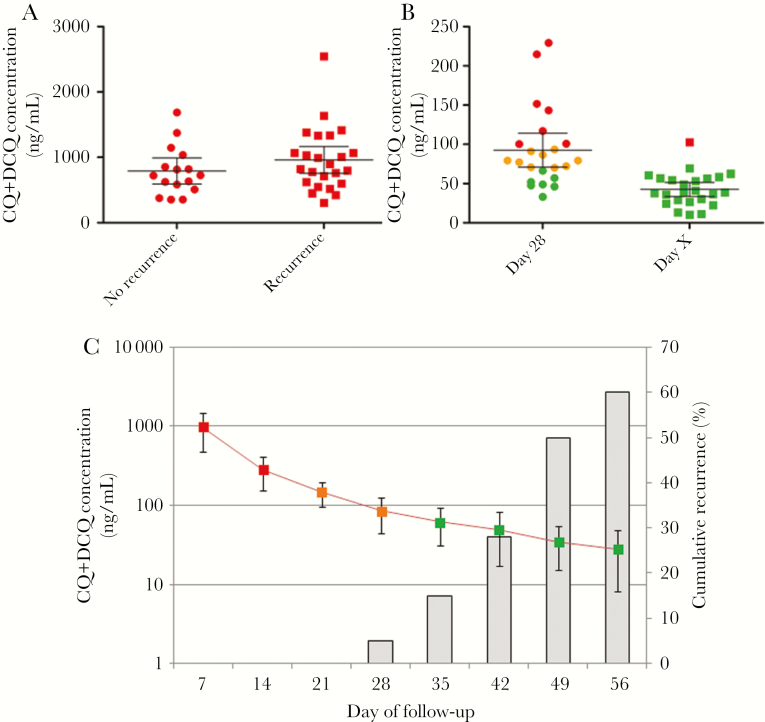
Results: P. vivax parasites were eliminated in all patients by day 3. Genomic analyses revealed that all clones in polyclonal infections were cleared at the same rate, indicating their equal susceptibility to CQ. CQ blood concentrations were below the therapeutic level in all recurrent infections (24 of 40 patients), which were efficiently cleared by a second course of CQ treatment. Genotyping (128 SNPs barcode) and sequences of entire parasite genome (Whole-Genome Sequencing, Illumina) indicated that two thirds (6 of 8) of the recurrent parasites resulted from heterologous relapses whose 50% are from by sibling/recombinant clones.
Conclusions: No evidence of CQ resistance was observed. Our data suggest that P. vivax antimalarial drug resistance is likely overestimated and that the current guidelines for clinical drug studies of P. vivax malaria need to be revised.
Figures

References
-
- World Health Organization. Methods for surveillance of antimalarial drug efficacy. In: Data WLC-i-P, ed, 2009.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
