

Understanding treatment guidelines with bismuth and non-bismuth quadruple Helicobacter pylori eradication therapies
- PMID: 30102559
- PMCID: PMC6309304
- DOI: 10.1080/14787210.2018.1511427
Understanding treatment guidelines with bismuth and non-bismuth quadruple Helicobacter pylori eradication therapies
Abstract
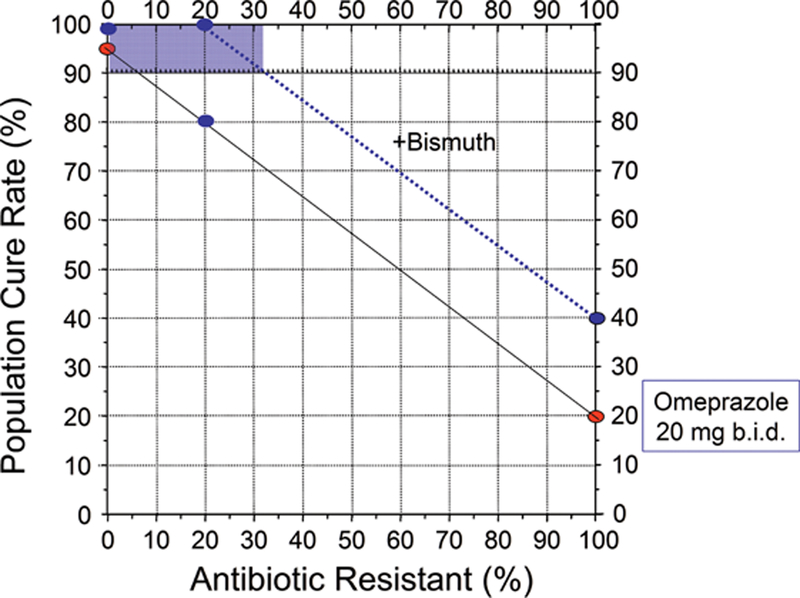
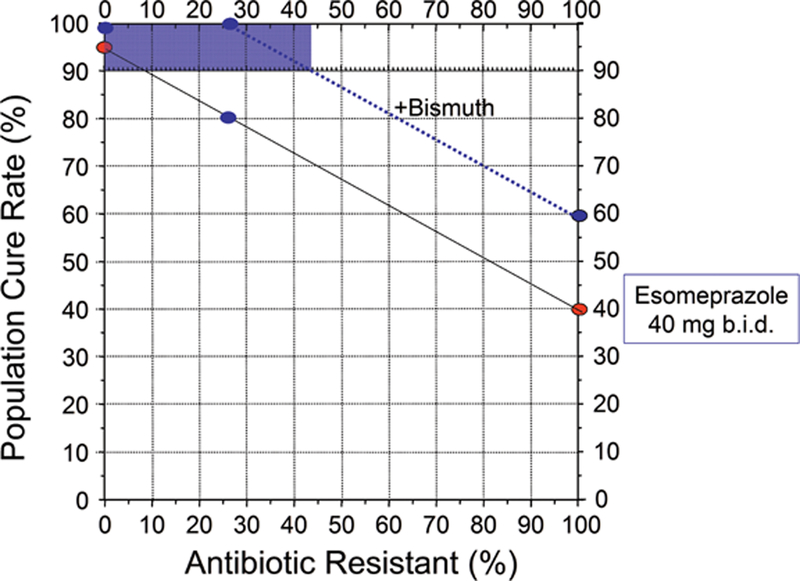
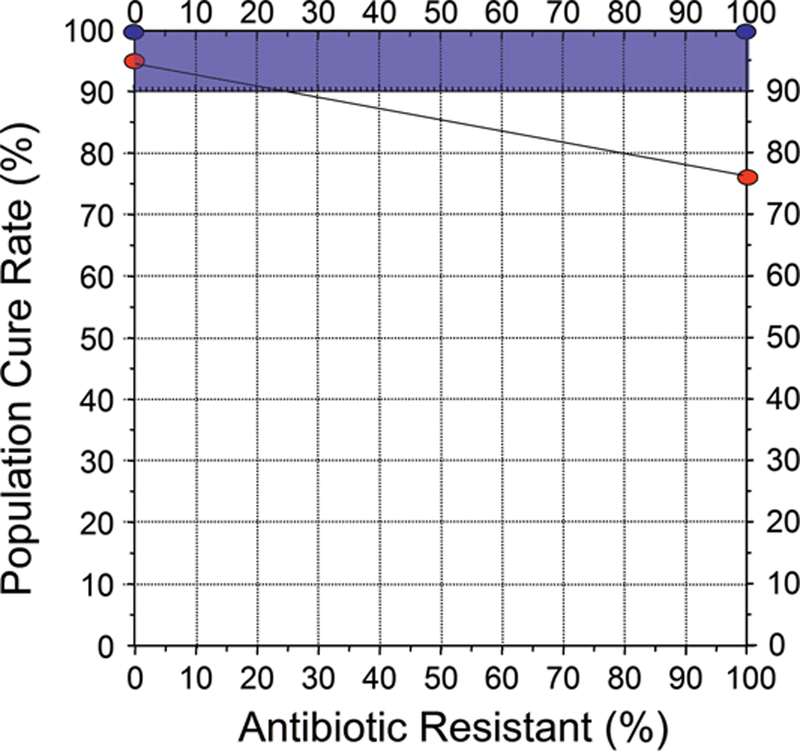
Recent Helicobacter pylori treatment guidelines recommend the 4-drug combinations bismuth quadruple therapy and concomitant therapy. Areas covered: We review antimicrobial therapy for H. pylori in the context of antimicrobial therapy in general and specifically in relation to good antimicrobial stewardship (defined as optimal selection, dose, and duration of an antimicrobial that results in the best clinical outcome for the treatment of infection, with minimal toxicity to the patient and minimal impact on subsequent resistance). Expert commentary: The lack of regional and local H. pylori susceptibility data prevents implementation of susceptibility-based antimicrobial therapy and forces compromises. Bismuth quadruple therapy employing at least 1,500 mg of metronidazole for 14 days is effective despite metronidazole resistance. The main drawback is side effects causing reduced adherence. Versions where amoxicillin replaces metronidazole or tetracycline also appear effective. It is likely that bismuth quadruple therapy can be simplified by giving bismuth and possibly tetracycline b.i.d., possibly with fewer side effects. Concomitant therapy (a proton pump inhibitor, metronidazole, clarithromycin, amoxicillin) is ineffective with dual clarithromycin-metronidazole resistance and all patients receive at least one unnecessary antibiotic thus promoting antimicrobial resistance worldwide. Concomitant therapy should be abandoned when susceptibility testing becomes widespread or an alternate becomes available.
Keywords: Amoxicillin; Helicobacter pylori; antibiotic misuse; antimicrobial stewardship; bismuth; clarithromycin; metronidazole; proton pump inhibitor; resistance; susceptibility; tetracycline; vonoprazan.
Conflict of interest statement
Declaration of interest
D Graham is a consultant for RedHill Biopharma regarding novel
Figures

References
-
- Dang BN, Graham DY. Helicobacter pylori infection and antibiotic resistance: a WHO high priority? Nat Rev Gastroenterol Hepatol. 2017;7: 383–384. - PMC - PubMed
-
*Emphasizes the recent World Health Organizations concern about global antimicrobial resistance and the organisms for which resistance is a major problem.
-
- Borsch GM, Graham DY. Helicobacter pylori In: Collen MJ, Benjamin SB, eds. Pharmacology of peptic ulcer disease, In: Handbook of Experimental Pharmacology Vol 99. Berlin: Springer-Verlag, 1991: 107–148.
-
*Comprehensive review of the early treatments tried for H. pylori infection
-
- Graham DY. Antibiotic resistance in Helicobacter pylori: implications for therapy. Gastroenterology 1998; 115: 1272–1277. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical