

High Operator and Hospital Volume Are Associated With a Decreased Risk of Death and Stroke After Carotid Revascularization: A Systematic Review and Meta-analysis
- PMID: 30102632
- PMCID: PMC6773608
- DOI: 10.1097/SLA.0000000000002880
High Operator and Hospital Volume Are Associated With a Decreased Risk of Death and Stroke After Carotid Revascularization: A Systematic Review and Meta-analysis
Abstract
Objective: To examine the association between operator or hospital volume and procedural outcomes of carotid revascularization.
Background: Operator and hospital volume have been proposed as determinants of outcome after carotid endarterectomy (CEA) or carotid artery stenting (CAS). The magnitude and clinical relevance of this relationship are debated.
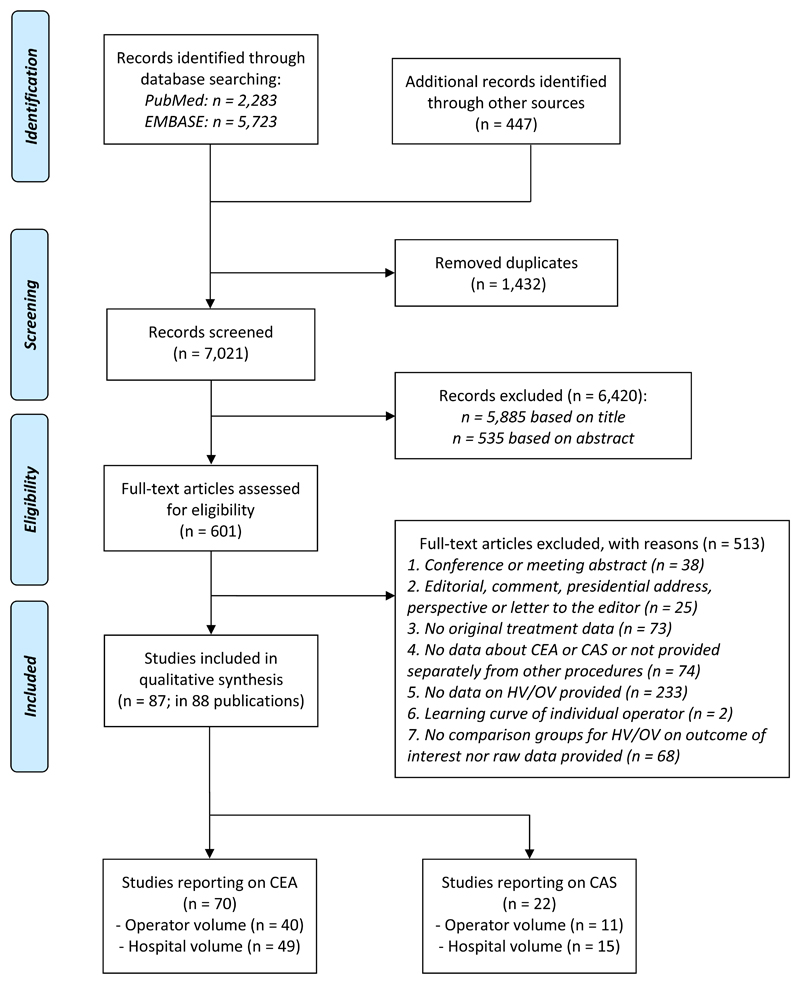
Methods: We systematically searched PubMed and EMBASE until August 21, 2017. The primary outcome was procedural (30 days, in-hospital, or perioperative) death or stroke. Obtained or estimated risk estimates were pooled with a generic inverse variance random-effects model.
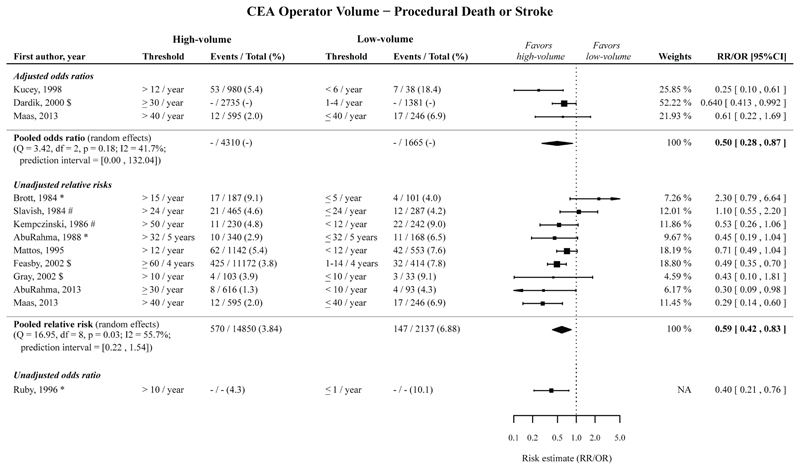
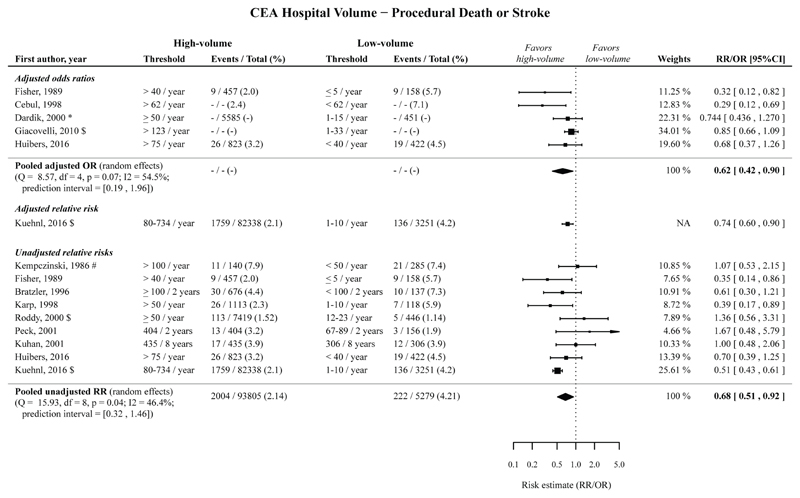
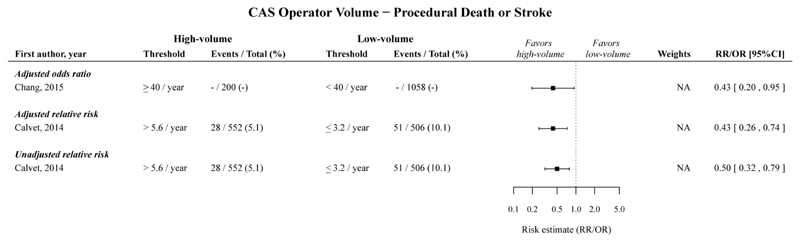
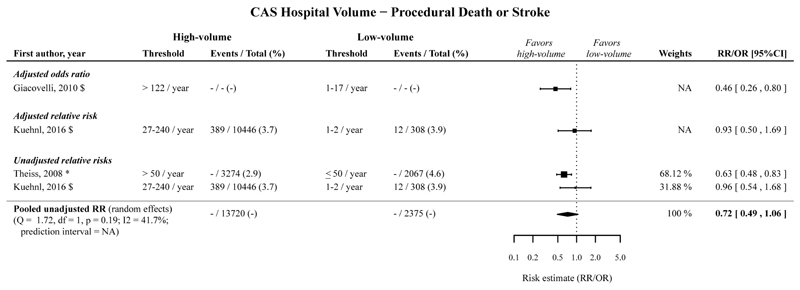
Results: We included 87 studies. A decreased risk of death or stroke following CEA was found for high compared to low operator volume with a pooled adjusted odds ratio (OR) of 0.50 (95% confidence interval [CI] 0.28-0.87; 3 cohorts), and a pooled unadjusted relative risk (RR) of 0.59 (95% CI 0.42-0.83; 9 cohorts); for high compared to low hospital volume with a pooled adjusted OR of 0.62 (95% CI 0.42-0.90; 5 cohorts), and a pooled unadjusted RR of 0.68 (95% CI 0.51-0.92; 9 cohorts). A decreased risk of death or stroke after CAS was found for high compared to low operator volume with an adjusted OR of 0.43 (95% CI 0.20-0.95; 1 cohort), and an unadjusted RR of 0.50 (95% CI 0.32-0.79; 1 cohort); for high compared to low hospital volume with an adjusted OR of 0.46 (95% CI 0.26-0.80; 1 cohort), and no significant decreased risk in a pooled unadjusted RR of 0.72 (95% CI 0.49-1.06; 2 cohorts).
Conclusions: We found a decreased risk of procedural death and stroke after CEA and CAS for high operator and high hospital volume, indicating that aiming for a high volume may help to reduce procedural complications.
Registration: This systematic review has been registered in the international prospective registry of systematic reviews (PROSPERO): CRD42017051491.
Conflict of interest statement
MHF: None
ECB: None
AH: None
RB: None
MB: None
GJdB: None
Figures
Comment in
-
Comment on "Problems With Investigating the Association Between Operator Volume, Hospital Volume, and Outcomes of Carotid Revascularization".Ann Surg. 2019 Aug;270(2):e50. doi: 10.1097/SLA.0000000000003116. Ann Surg. 2019. PMID: 30499805 No abstract available.
-
Response to Comment on "High Operator and Hospital Volume are Associated With a Decreased Risk of Death and Stroke Following Carotid Revascularization: A Systematic Review and Meta-analysis: Authors' Reply".Ann Surg. 2019 Aug;270(2):e50-e51. doi: 10.1097/SLA.0000000000003118. Ann Surg. 2019. PMID: 30499811 No abstract available.
-
Comment on "Meta-analysis of Effect of Volume (Hospital and Operator) on Carotid Revascularization Outcomes".Ann Surg. 2019 Dec;270(6):e133-e134. doi: 10.1097/SLA.0000000000003414. Ann Surg. 2019. PMID: 31205062 No abstract available.
-
Response to the Comment on "Meta-analysis of Effect of Volume (Hospital and Operator) on Carotid Revascularization Outcomes".Ann Surg. 2021 Jul 1;274(1):e107. doi: 10.1097/SLA.0000000000003411. Ann Surg. 2021. PMID: 31268898 No abstract available.
References
-
- Rerkasem K, Rothwell PM. Carotid endarterectomy for symptomatic carotid stenosis. Cochrane Database Syst Rev. 2011 CD001081. - PubMed
-
- Jacobowitz GR, Rockman CB, Lamparello PJ, et al. Causes of perioperative stroke after carotid endarterectomy: special considerations in symptomatic patients. Ann Vasc Surg. 2001;15:19–24. - PubMed
-
- Riles TS, Imparato AM, Jacobowitz GR, et al. The cause of perioperative stroke after carotid endarterectomy. J Vasc Surg. 1994;19:206–214. - PubMed
-
- de Borst GJ, Moll FL, van de Pavoordt HD, et al. Stroke from carotid endarterectomy: when and how to reduce perioperative stroke rate? Eur J Vasc Endovasc Surg. 2001;21:484–489. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
