

Dual targeting: Combining costimulation blockade and bortezomib to permit kidney transplantation in sensitized recipients
- PMID: 30102844
- PMCID: PMC7185755
- DOI: 10.1111/ajt.15067
Dual targeting: Combining costimulation blockade and bortezomib to permit kidney transplantation in sensitized recipients
Abstract
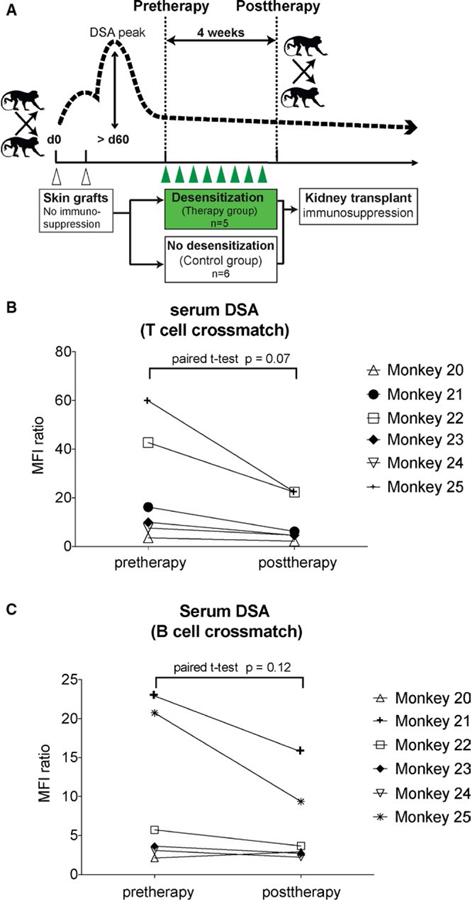
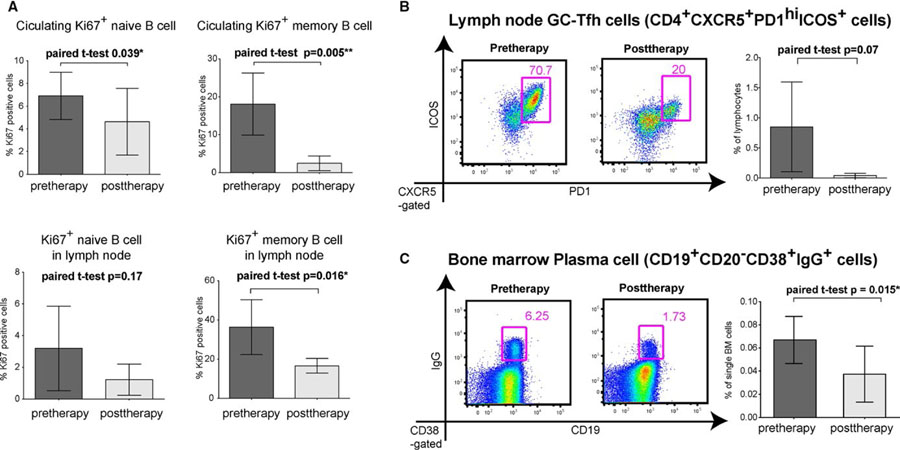
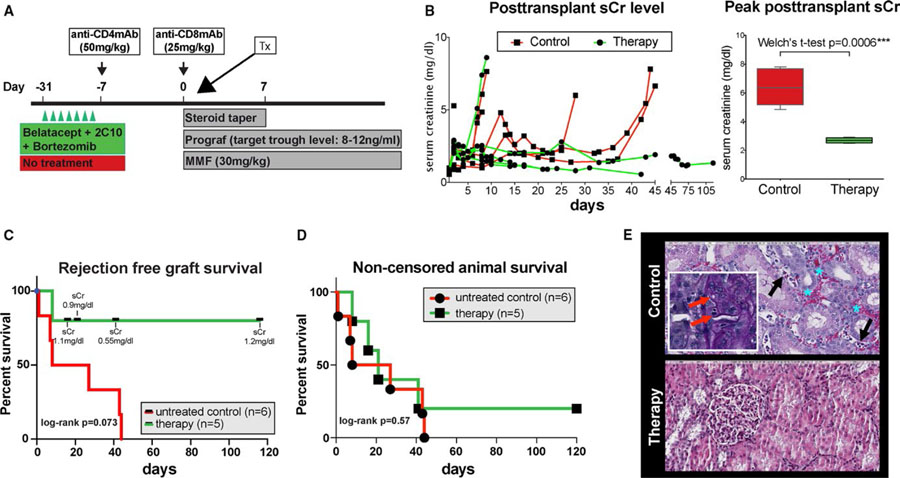
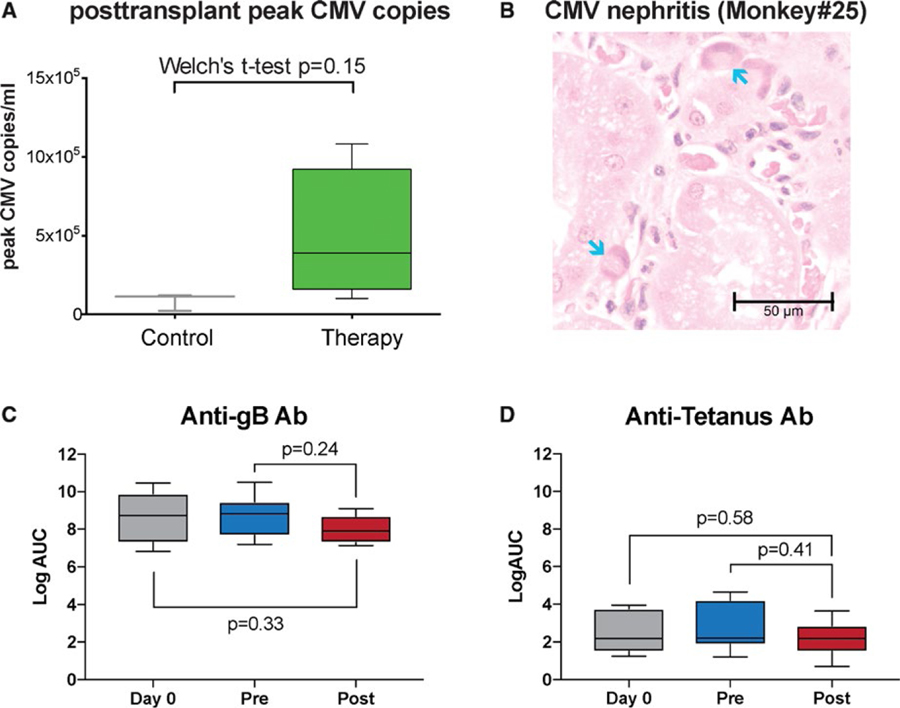
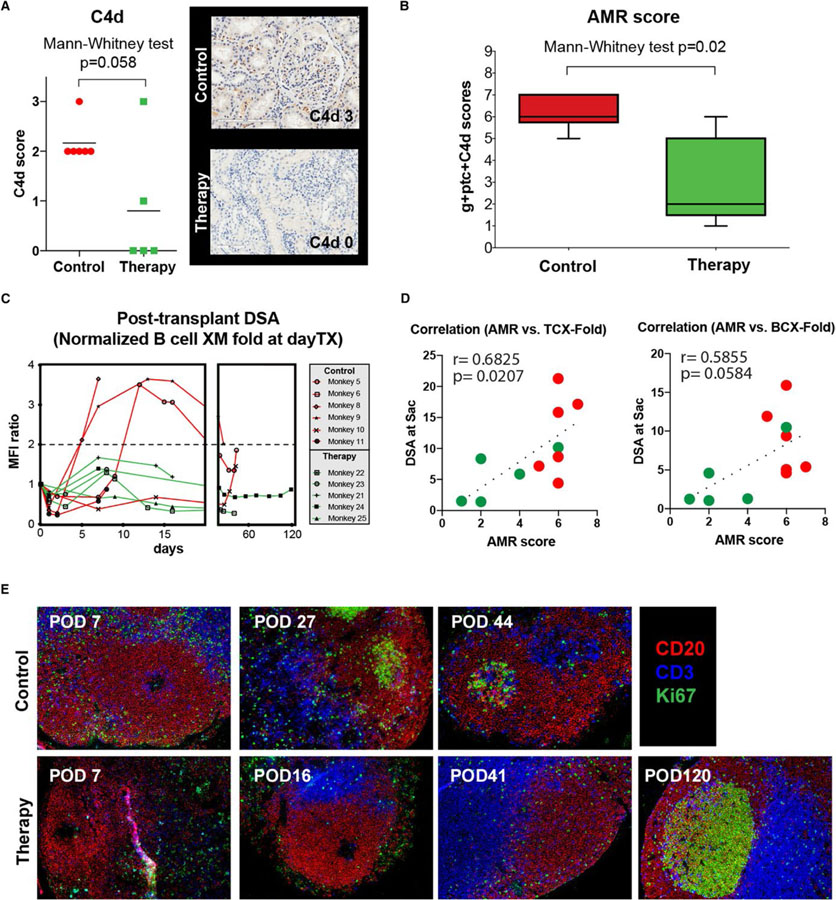
Previous evidence suggests that a homeostatic germinal center (GC) response may limit bortezomib desensitization therapy. We evaluated the combination of costimulation blockade with bortezomib in a sensitized non-human primate kidney transplant model. Sensitized animals were treated with bortezomib, belatacept, and anti-CD40 mAb twice weekly for a month (n = 6) and compared to control animals (n = 7). Desensitization therapy-mediated DSA reductions approached statistical significance (P = .07) and significantly diminished bone marrow PCs, lymph node follicular helper T cells, and memory B cell proliferation. Graft survival was prolonged in the desensitization group (P = .073). All control animals (n = 6) experienced graft loss due to antibody-mediated rejection (AMR) after kidney transplantation, compared to one desensitized animal (1/5). Overall, histological AMR scores were significantly lower in the treatment group (n = 5) compared to control (P = .020). However, CMV disease was common in the desensitized group (3/5). Desensitized animals were sacrificed after long-term follow-up with functioning grafts. Dual targeting of both plasma cells and upstream GC responses successfully prolongs graft survival in a sensitized NHP model despite significant infectious complications and drug toxicity. Further work is planned to dissect underlying mechanisms, and explore safety concerns.
Keywords: alloantibody; animal models: nonhuman primate; basic (laboratory) research/science; desensitization; immunosuppressant - fusion proteins and monoclonal antibodies: costimulation molecule specific; immunosuppression/immune modulation; kidney transplantation/nephrology; plasma cells.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
DISCLOSURE
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
-
- Gloor JM, DeGoey SR, Pineda AA, et al. Overcoming a positive crossmatch in living-donor kidney transplantation. Am J Transplant. 2003;3(8):1017–1023. - PubMed
-
- Riella LV, Safa K, Yagan J, et al. Long-term outcomes of kidney transplantation across a positive complement-dependent cytotoxicity crossmatch. Transplantation. 2014;97(12):1247–1252. - PubMed
-
- Bartel G, Wahrmann M, Regele H, et al. Peritransplant immunoadsorption for positive crossmatch deceased donor kidney transplantation. Am J Transplant. 2010;10(9):2033–2042. - PubMed
-
- Gloor JM, Winters JL, Cornell LD, et al. Baseline donor-specific antibody levels and outcomes in positive crossmatch kidney transplantation. Am J Transplant. 2010;10(3):582–589. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
