

Prominent Non-Memory Deficits in Alzheimer's Disease Are Associated with Faster Disease Progression
- PMID: 30103316
- PMCID: PMC6588161
- DOI: 10.3233/JAD-171088
Prominent Non-Memory Deficits in Alzheimer's Disease Are Associated with Faster Disease Progression
Abstract
Background: Alzheimer's disease (AD) is a heterogeneous disorder.
Objective: To investigate whether cognitive AD subtypes are associated with different rates of disease progression.
Methods: We included 1,066 probable AD patients from the Amsterdam Dementia Cohort (n = 290), Alzheimer's Disease Neuroimaging Initiative (n = 268), Dementia Competence Network (n = 226), and University of California, San Francisco (n = 282) with available follow-up data. Patients were previously clustered into two subtypes based on their neuropsychological test results: one with most prominent memory impairment (n = 663) and one with most prominent non-memory impairment (n = 403). We examined associations between cognitive subtype and disease progression, as measured with repeated Mini-Mental State Examination (MMSE) and Clinical Dementia Rating scale sum of boxes (CDR sob), using linear mixed models. Furthermore, we investigated mortality risk associated with subtypes using Cox proportional hazard analyses.
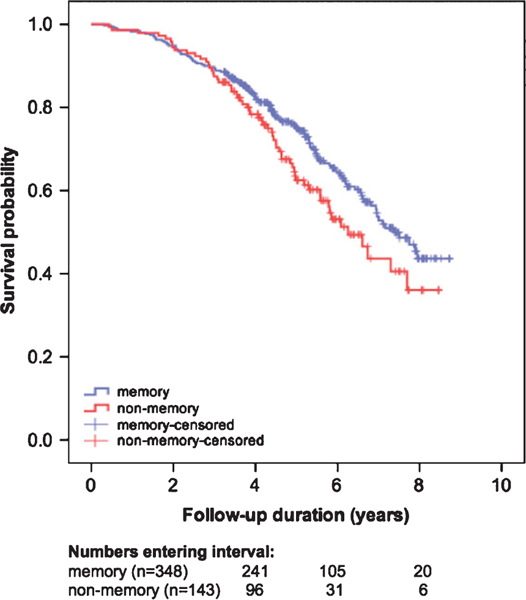
Results: Patients were 71±9 years old; 541 (51%) were female. At baseline, pooled non-memory patients had worse MMSE scores (23.1±0.1) and slightly worse CDR sob (4.4±0.1) than memory patients (MMSE 24.0±0.1; p < 0.001; CDR sob 4.1±0.1; p < 0.001). During follow-up, pooled non-memory patients showed steeper annual decline in MMSE (-2.8±0.1) and steeper annual increase in CDR sob (1.8±0.1) than memory patients (MMSE - 1.9±0.1; pinteraction<0.001; CDR sob 1.3±0.1; pinteraction<0.001). Furthermore, the non-memory subtype was associated with an increased risk of mortality compared with the memory subtype at trend level (HR = 1.36, CI = 1.00-1.85, p = 0.05).
Conclusions: AD patients with most prominently non-memory impairment show faster disease progression and higher risk of mortality than patients with most prominently memory impairment.
Keywords: Alzheimer’s disease; clustering; cognition; dementia; disease progression; mortality; phenotypes; subtypes.
Figures

References
-
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Scheltens P, Carrillo MC, Thies B, Weintraub S, Phelps CH (2011) The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 3, 263–269. - PMC - PubMed
-
- Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, Ogar JM, Rohrer JD, Black S, Boeve BF, Manes F, Dronkers NF, Vandenberghe R, Rascovsky K, Patterson K, Miller BL, Knopman DS, Hodges JR, Mesulam MM, Grossman M (2011) Classification of primary progressive aphasia and its variants. Neurology 11, 1006–1014. - PMC - PubMed
-
- Benson DF, Davis RJ, Snyder BD (1988) Posterior cortical atrophy. Arch Neurol 45, 789–793. - PubMed
-
- Ossenkoppele R, Pijnenburg YAL, Perry DC, Cohn-Sheehy BI, Scheltens NME, Vogel JW, Kramer JH, van der Vlies AE, La Joie R, Rosen HJ, van der Flier WM, Grinberg LT, Rozemuller AJ, Huang EJ, van Berckel BNM, Miller BL, Barkhof F, Jagust WJ, Scheltens P, Seeley WW, Rabi-novici GD (2015) The behavioural/dysexecutive variant of Alzheimer’s disease: Clinical, neuroimaging and pathological features. Brain 138, 2732–2749. - PMC - PubMed
-
- Van Der Flier WM, Schoonenboom SNM, Pijnenburg YAL, Fox NC, Scheltens P (2006) The effect of APOE genotype on clinical phenotype in Alzheimer disease. Neurology 67, 526–527. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
