

Effect of Patiromer in Hyperkalemic Patients Taking and Not Taking RAAS Inhibitors
- PMID: 30103622
- PMCID: PMC6193203
- DOI: 10.1177/1074248418788334
Effect of Patiromer in Hyperkalemic Patients Taking and Not Taking RAAS Inhibitors
Abstract
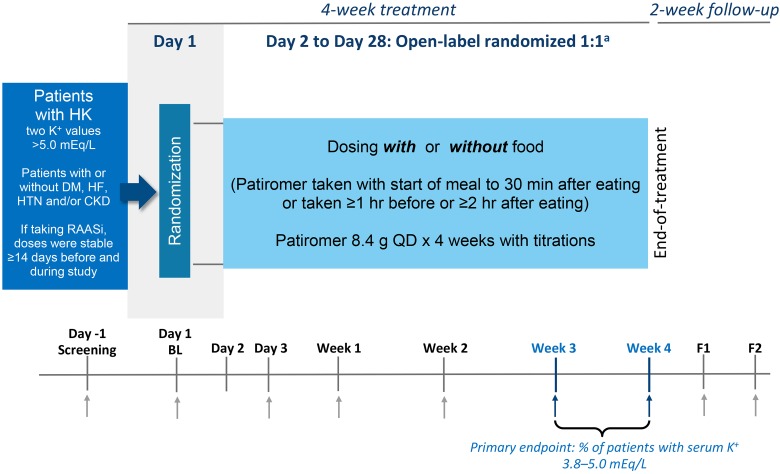
Introduction: Hyperkalemia (potassium >5.0 mEq/L) affects heart failure patients with renal disease regardless of the use of renin-angiotensin-aldosterone system inhibitors (RAASi). The open-label TOURMALINE study showed that patiromer, a sodium-free, nonabsorbed potassium binder, lowers serum potassium of hyperkalemic patients similarly when given with or without food; unlike prior studies, patients were not required to be taking RAASi. We conducted post hoc analyses to provide the first report of patiromer in patients not taking RAASi.
Methods: Hyperkalemic patients received patiromer, 8.4 g/d to start, adjusted to achieve and maintain serum potassium of 3.8 to 5.0 mEq/L. If taking RAASi, stable doses were required. The primary end point was the proportion of patients with serum potassium 3.8 to 5.0 mEq/L at week 3 or 4. This analysis presents data by patients taking or not taking RAASi.
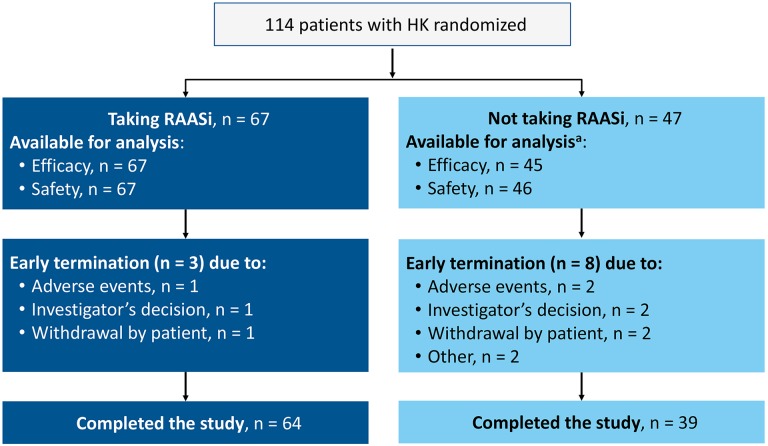
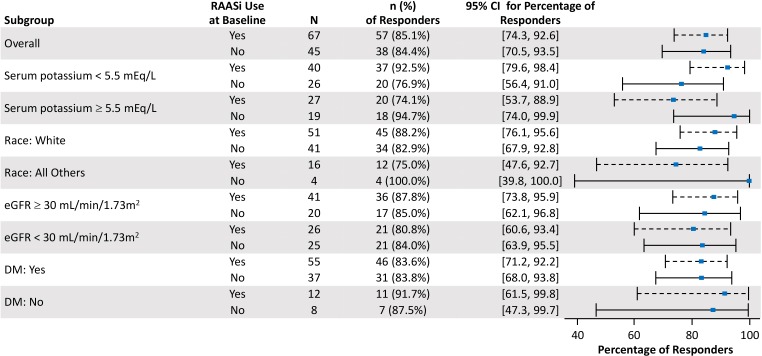
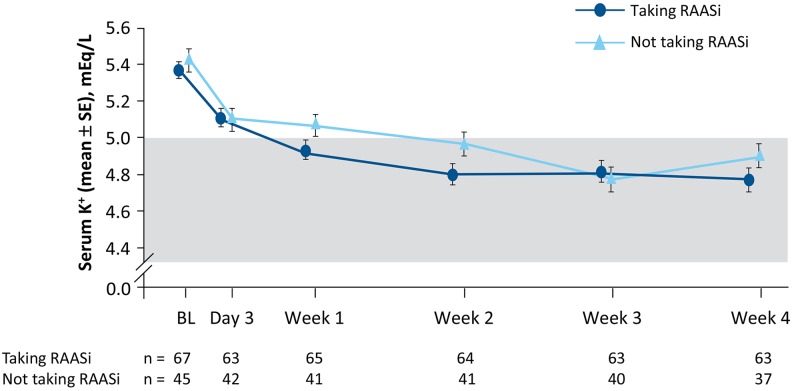
Results: Demographics and baseline characteristics were similar in patients taking (n = 67) and not taking RAASi (n = 45). Baseline mean (SD) serum potassium was 5.37 (0.37) mEq/L and 5.42 (0.43) mEq/L in patients taking and not taking RAASi, respectively. Mean (SD) daily patiromer doses were similar (10.7 [3.2] and 11.5 [4.0] g, respectively). The primary end point was achieved in 85% (95% confidence interval [CI]: 74-93) of patients taking RAASi and in 84% (95% CI: 71-94) of patients not taking RAASi. From baseline to week 4, the mean (SE) change in serum potassium was -0.67 (0.08) mEq/L in patients taking RAASi and -0.56 (0.10) mEq/L in patients not taking RAASi (both P < .0001 vs baseline, P = nonsignificant between groups). Adverse events were reported in 26 (39%) patients taking RAASi and 25 (54%) not taking RAASi; the most common adverse event was diarrhea (2% and 11%, respectively; no cases were severe). Five patients (2 taking RAASi) reported 6 serious adverse events; none considered related to patiromer.
Conclusions: Patiromer was effective and generally well-tolerated for hyperkalemia treatment, whether or not patients were taking RAAS inhibitors.
Keywords: RAAS inhibitor; chronic kidney disease; heart failure; hyperkalemia; patiromer.
Conflict of interest statement
Figures
References
-
- Nilsson E, Gasparini A, Arnlov J, et al. Incidence and determinants of hyperkalemia and hypokalemia in a large healthcare system. Int J Cardiol. 2017;245:277–284. - PubMed
-
- Weir MR, Rolfe M. Potassium homeostasis and renin-angiotensin-aldosterone system inhibitors. Clin J Am Soc Nephrol. 2010;5(3):531–548. - PubMed
-
- Balamuthusamy S, Srinivasan L, Verma M, et al. Renin angiotensin system blockade and cardiovascular outcomes in patients with chronic kidney disease and proteinuria: a meta-analysis. Am Heart J. 2008;155(5):791–805. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
