

Catheter ablation for treatment of patients with atrial fibrillation and heart failure: a meta-analysis of randomized controlled trials
- PMID: 30103676
- PMCID: PMC6090632
- DOI: 10.1186/s12872-018-0904-3
Catheter ablation for treatment of patients with atrial fibrillation and heart failure: a meta-analysis of randomized controlled trials
Abstract
Background: There is a little evidence for the effects of catheter ablation (CA) on hard endpoints in patients with atrial fibrillation (AF) and heart failure (HF).
Methods: PubMed, Embase and Cochrane Library were searched for randomized controlled trials (RCTs) enrolling patients with AF and HF who were assigned to CA, rate control or medical rhythm control groups. This meta-analysis was performed by using random-effect models.
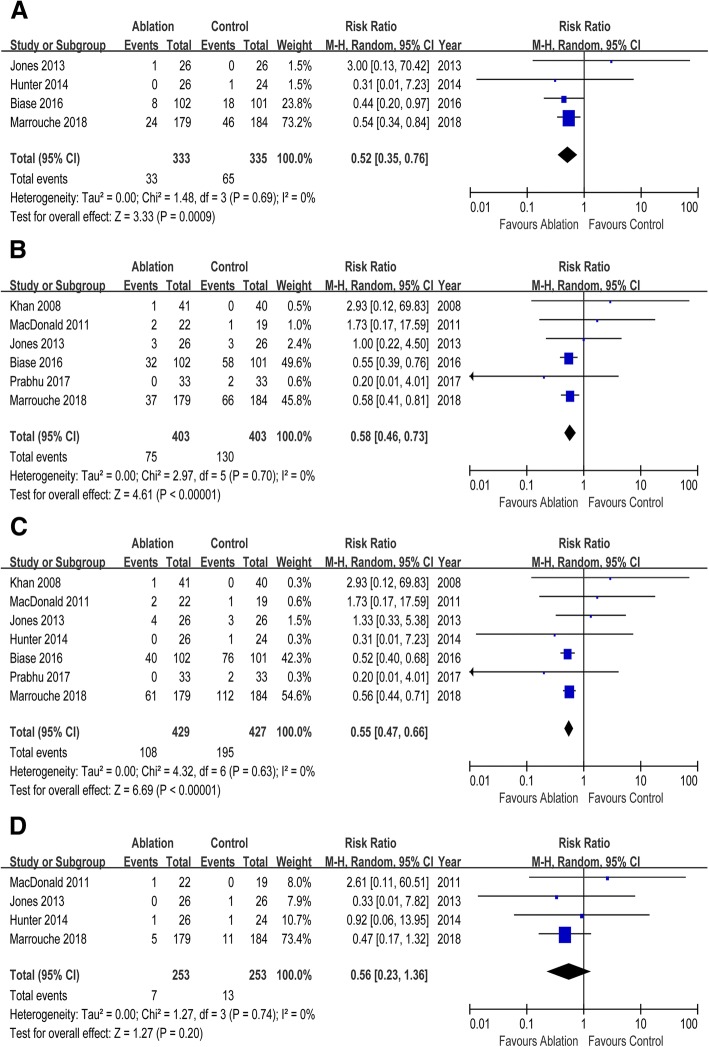
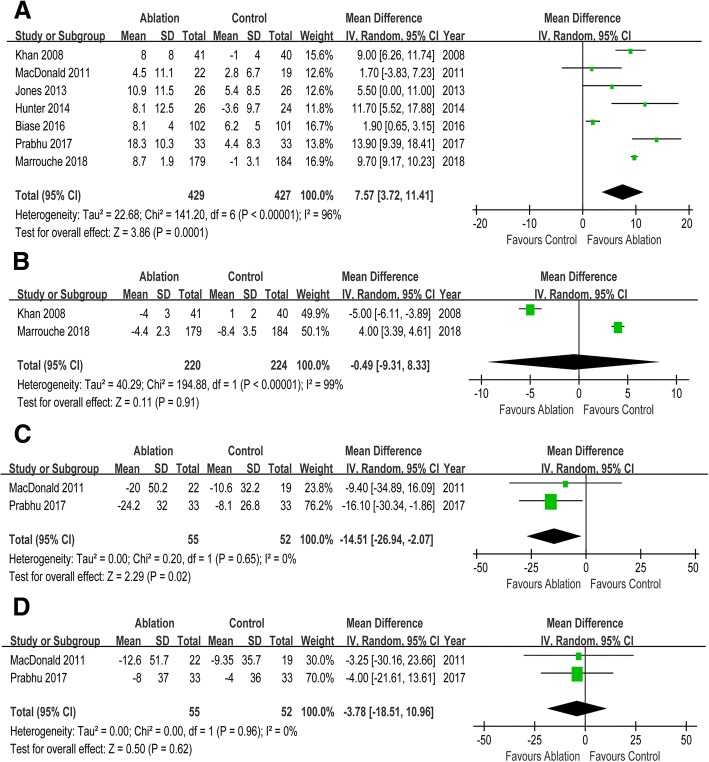
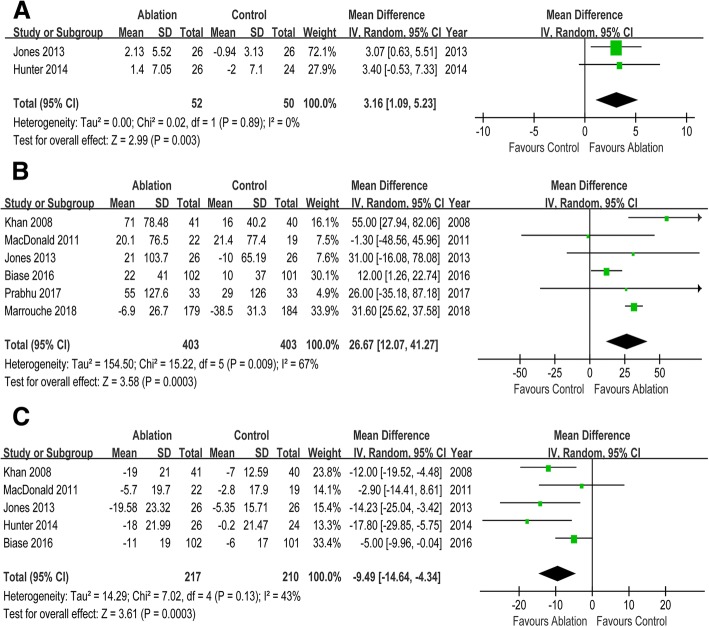
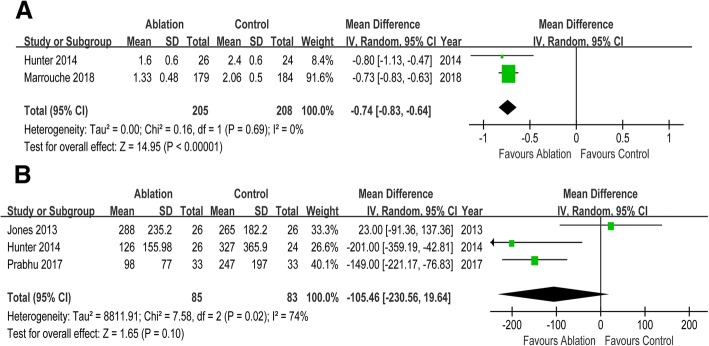
Results: Seven RCTs enrolling 856 participants were included in this meta-analysis. CA reduced the risks of all-cause mortality (risk ratio [RR] 0.52, 95% CI 0.35 to 0.76), HF readmission (RR 0.58, 95% CI 0.46 to 0.66) and the composite of all-cause mortality and HF readmission (RR 0.55, 95% CI 0.47 to 0.66) when compared with control. But there was no significant difference in cerebrovascular accident (RR 0.56, 95% CI 0.23 to 1.36) between two groups. Compared with control, CA was associated with improvement in left ventricular ejection fraction (mean difference [MD] 7.57, 95% CI 3.72 to 11.41), left ventricular end systolic volume (MD -14.51, 95% CI -26.84 to - 2.07), and left ventricular end diastolic volume (MD -3.78, 95% CI -18.51 to 10.96). Patients undergoing CA exhibited increased peak oxygen consumption (MD 3.16, 95% CI 1.09 to 5.23), longer 6-min walk test distance (MD 26.67, 95% CI 12.07 to 41.27), and reduced Minnesota Living with Heart Failure Questionnaire scores (MD -9.49, 95% CI -14.64 to - 4.34) than those in control group. Compared with control, CA was associated with improved New York Heart Association class (MD -0.74, 95% CI -0.83 to - 0.64) and lower B-type natriuretic peptide levels (MD -105.96, 95% CI -230.56 to 19.64).
Conclusions: CA was associated with improved survival, morphologic changes, functional capacity and quality of life relative to control. CA should be considered in patients with AF and HF.
Keywords: Atrial fibrillation; Catheter ablation; Heart failure; Rate control strategy; Rhythm control strategy.
Conflict of interest statement
Not applicable. (Because this is a meta-analysis).
Not applicable.
The authors declare that they have no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Efficacy of catheter ablation for atrial fibrillation in heart failure: a meta-analysis of randomized controlled trials.ESC Heart Fail. 2024 Oct;11(5):2684-2693. doi: 10.1002/ehf2.14814. Epub 2024 Apr 25. ESC Heart Fail. 2024. PMID: 38661235 Free PMC article.
-
Catheter Ablation of Atrial Fibrillation in Patients With Heart Failure: A Meta-analysis of Randomized Controlled Trials.Ann Intern Med. 2019 Jan 1;170(1):41-50. doi: 10.7326/M18-0992. Epub 2018 Dec 25. Ann Intern Med. 2019. PMID: 30583296
-
Catheter Ablation Versus Medical Therapy for Atrial Fibrillation in Patients With Heart Failure: A Meta-Analysis of Randomised Controlled Trials.Heart Lung Circ. 2019 May;28(5):707-718. doi: 10.1016/j.hlc.2018.10.022. Epub 2018 Nov 17. Heart Lung Circ. 2019. PMID: 30509786 Review.
-
Catheter ablation for atrial fibrillation in heart failure with reduced ejection fraction patients: A meta-analysis.Heart Rhythm. 2024 Sep;21(9):1604-1612. doi: 10.1016/j.hrthm.2024.04.098. Epub 2024 May 3. Heart Rhythm. 2024. PMID: 38705438
-
Catheter ablation for atrial fibrillation in heart failure with reduced ejection fraction: a systematic review and meta-analysis of randomized controlled trials.BMC Cardiovasc Disord. 2019 Jan 15;19(1):18. doi: 10.1186/s12872-019-0998-2. BMC Cardiovasc Disord. 2019. PMID: 30646857 Free PMC article.
Cited by
-
Methodological and Clinical Heterogeneity and Extraction Errors in Meta-Analyses of Catheter Ablation for Atrial Fibrillation in Heart Failure.J Am Heart Assoc. 2019 Nov 5;8(21):e013779. doi: 10.1161/JAHA.119.013779. Epub 2019 Oct 18. J Am Heart Assoc. 2019. PMID: 31625420 Free PMC article.
-
Tackling Patient-Reported Outcomes in Atrial Fibrillation and Heart Failure: Identifying Disease-Specific Symptoms?Cardiol Clin. 2019 May;37(2):139-146. doi: 10.1016/j.ccl.2019.01.013. Cardiol Clin. 2019. PMID: 30926015 Free PMC article. Review.
-
Optimal effectiveness of heart failure management - an umbrella review of meta-analyses examining the effectiveness of interventions to reduce (re)hospitalizations in heart failure.Heart Fail Rev. 2022 Sep;27(5):1683-1748. doi: 10.1007/s10741-021-10212-8. Epub 2022 Mar 3. Heart Fail Rev. 2022. PMID: 35239106 Free PMC article.
-
Assessment of Redundant Meta-Analyses on Catheter Ablation of Atrial Fibrillation in Patients with Heart Failure.Rev Cardiovasc Med. 2024 Nov 21;25(11):418. doi: 10.31083/j.rcm2511418. eCollection 2024 Nov. Rev Cardiovasc Med. 2024. PMID: 39618855 Free PMC article.
-
Predictors of Atrial Fibrillation Recurrences after a First Radiofrequency Catheter Ablation Intervention for Paroxysmal Atrial Fibrillation-Experience of a Low Volume Ablation Centre.Medicina (Kaunas). 2021 Oct 20;57(11):1139. doi: 10.3390/medicina57111139. Medicina (Kaunas). 2021. PMID: 34833357 Free PMC article.
References
-
- Mogensen UM, Jhund PS, Abraham WT, Desai AS, Dickstein K, Packer M, Rouleau JL, Solomon SD, Swedberg K, Zile MR, et al. Type of atrial fibrillation and outcomes in patients with heart failure and reduced ejection fraction. J Am Coll Cardiol. 2017;70(20):2490–2500. doi: 10.1016/j.jacc.2017.09.027. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
