

Impact of missing individual patient data on 18 meta-analyses of randomised trials in oncology: Gustave Roussy experience
- PMID: 30104312
- PMCID: PMC6091903
- DOI: 10.1136/bmjopen-2017-020499
Impact of missing individual patient data on 18 meta-analyses of randomised trials in oncology: Gustave Roussy experience
Abstract
Objective: To compare the characteristics, quality and treatment effects of randomised clinical trials (RCTs) by individual patient data (IPD) availability, in trials eligible for 18 IPD meta-analyses (MA).
Design: Trial characteristics, risk of bias (RoB) and hazard ratio (HR) for overall survival were extracted from IPD-MA publications and/or RCTs publications. Data for the RoB assessment were extracted for a subset of 73 RCTs. Two investigators blinded to whether IPD was available or not evaluated the RoB for these trials. Treatment effects were compared using ratios of global HRs (RHRs) of IPD-unavailable trials and IPD-available trials. RHR were pooled using a fixed-effect model.
Data sources: We examined the IPD availability for each trial eligible for each IPD-MA; when the IPD was not available for a trial, we used information from published sources.
Eligibility criteria for selecting studies: We selected all published IPD-MAs conducted at Gustave Roussy and the RCTs eligible for each.
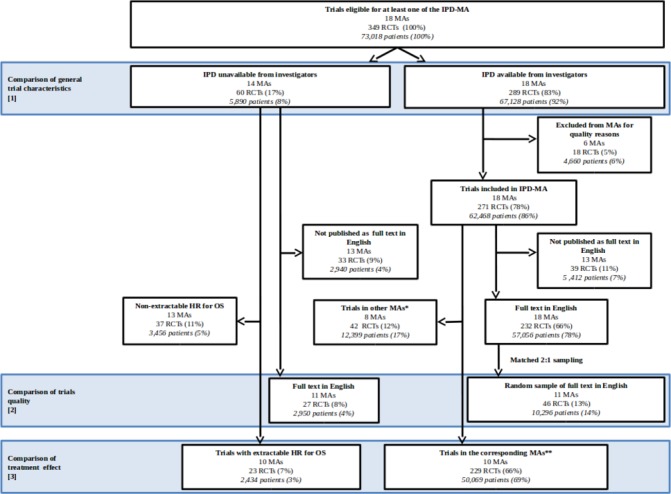
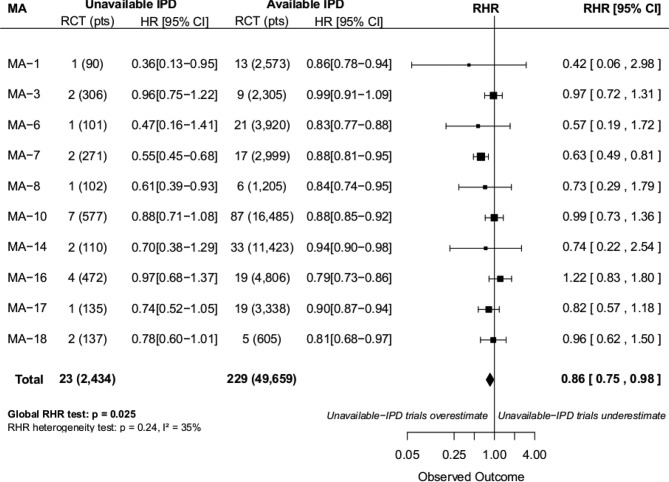
Results: 349 RCTs (73 018 patients) from 18 MAs were eligible: 60 RCTs (5890 patients) had unavailable IPD and 289 RCTs (67 128 patients) had available IPD. The main reason for IPD unavailability was data loss by investigators. IPD-unavailable trials were smaller (p<0.001), more often monocentric (p<0.001) and non-international (p=0.0004) than IPD-available trials. Geographical areas differed (p=0.054) between IPD-unavailable IPD-available trials. RoB was higher in IPD-unavailable RCTs for random sequence generation (p=0.007) and allocation concealment (p=0.006). The HR and 95% confidence interval (CI) for overall survival were extractable from publications in 23/60 IPD-unavailable trials included in 10 different MAs. Treatment effects were significantly greater for IPD-unavailable trials compared with IPD-available trials (RHR=0.86 (95% CI 0.75 to 0.98)).
Conclusions: IPD-unavailable RCTs were significantly different from IPD-available RCTs in terms of trial characteristics and were at greater RoB. IPD-unavailable RCTs had a significantly greater treatment effect.
Keywords: individual patient data; meta-analysis; missing data; quality; randomized clinical trials; risk of bias.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
No consistent evidence of data availability bias existed in recent individual participant data meta-analyses: a meta-epidemiological study.J Clin Epidemiol. 2020 Feb;118:107-114.e5. doi: 10.1016/j.jclinepi.2019.10.004. Epub 2019 Oct 22. J Clin Epidemiol. 2020. PMID: 31654789
-
To share or not to share data: how valid are trials evaluating first-line ovulation induction for polycystic ovary syndrome?Hum Reprod Update. 2020 Nov 1;26(6):929-941. doi: 10.1093/humupd/dmaa031. Hum Reprod Update. 2020. PMID: 32935841
-
Comparison of aggregate and individual participant data approaches to meta-analysis of randomised trials: An observational study.PLoS Med. 2020 Jan 31;17(1):e1003019. doi: 10.1371/journal.pmed.1003019. eCollection 2020 Jan. PLoS Med. 2020. PMID: 32004320 Free PMC article.
-
The methodological quality of individual participant data meta-analysis on intervention effects: systematic review.BMJ. 2021 Apr 19;373:n736. doi: 10.1136/bmj.n736. BMJ. 2021. PMID: 33875446 Free PMC article.
-
Updating insights into rosiglitazone and cardiovascular risk through shared data: individual patient and summary level meta-analyses.BMJ. 2020 Feb 5;368:l7078. doi: 10.1136/bmj.l7078. BMJ. 2020. PMID: 32024657 Free PMC article.
Cited by
-
Meta-analysis of chemotherapy in nasopharynx carcinoma (MAC-NPC): An update on 26 trials and 7080 patients.Clin Transl Radiat Oncol. 2021 Nov 26;32:59-68. doi: 10.1016/j.ctro.2021.11.007. eCollection 2022 Jan. Clin Transl Radiat Oncol. 2021. PMID: 34935776 Free PMC article.
-
Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 107 randomized trials and 19,805 patients, on behalf of MACH-NC Group.Radiother Oncol. 2021 Mar;156:281-293. doi: 10.1016/j.radonc.2021.01.013. Epub 2021 Jan 27. Radiother Oncol. 2021. PMID: 33515668 Free PMC article.
-
Current Issues on Research Conducted to Improve Women's Health.Healthcare (Basel). 2021 Jan 17;9(1):92. doi: 10.3390/healthcare9010092. Healthcare (Basel). 2021. PMID: 33477390 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases