Ultrasound-guided adductor canal block versus femoral nerve block for arthroscopic anterior cruciate ligament repair under general anesthesia
- PMID: 30104837
- PMCID: PMC6066890
- DOI: 10.4103/joacp.JOACP_172_17
Ultrasound-guided adductor canal block versus femoral nerve block for arthroscopic anterior cruciate ligament repair under general anesthesia
Abstract
Background and aims: Adductor canal block (ACB) is now an established component of multimodal analgesia for knee replacement surgery and is slowly replacing femoral nerve block (FNB). It is also gaining popularity for providing pain relief in knee arthroscopies including anterior cruciate ligament reconstruction surgery (ACLR). Data is lacking from the Indian subcontinent on comparing ACB to the traditional FNB for ACLR. Hence, we conducted the present study to compare ACB and FNB in ACLR under general anesthesia.
Material and methods: Sixty patients were randomized to receive either ACB or FNB under ultrasound guidance. Postoperatively, quadriceps muscle strength (straight leg raise and time up and go; TUG test) and quality of analgesia (numeric rating scale; NRS and patient satisfaction score) were assessed every 6 hour, and thereafter, up to 48 hours. The time of rescue analgesia and total analgesic consumption (tramadol) were also recorded. Data was statistically analyzed and P < 0.05 was considered to be significant.
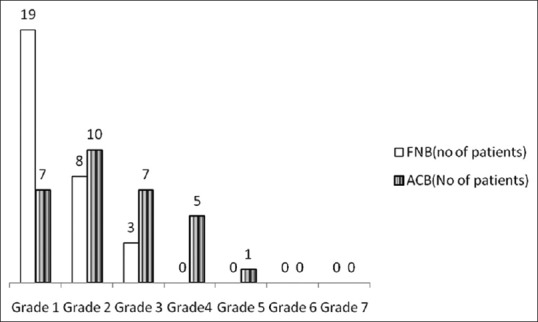
Results: Patients receiving ACB had significantly less quadriceps weakness (P < 0.001) compared to FNB on postoperative day (POD) 1. In addition, patient satisfaction score was statistically higher (P < 0.05) in FNB on POD1. Both the above parameters were comparable on POD2. No statistically significant difference was recorded in NRS, time for rescue analgesia, and total analgesic consumption among the two groups.
Conclusion: ACB preserves quadriceps motor strength while providing analgesia comparable to FNB in patients undergoing ACLR. However, patient satisfaction score is better with FNB than ACB.
Keywords: Adductor canal block; arthroscopic ACLR; femoral nerve block.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Effect of Adductor Canal Block Versus Femoral Nerve Block on Quadriceps Strength, Function, and Postoperative Pain After Anterior Cruciate Ligament Reconstruction: A Systematic Review of Level 1 Studies.Am J Sports Med. 2020 Jul;48(9):2305-2313. doi: 10.1177/0363546519883589. Epub 2019 Dec 4. Am J Sports Med. 2020. PMID: 31800300
-
Comparative Study of Adductor Canal Block and Femoral Nerve Block for Postoperative Analgesia After Arthroscopic Anterior Cruciate Ligament Tear Repair Surgeries.Cureus. 2022 Apr 10;14(4):e24007. doi: 10.7759/cureus.24007. eCollection 2022 Apr. Cureus. 2022. PMID: 35547414 Free PMC article.
-
Adductor Canal Versus Femoral Nerve Block after Anterior Cruciate Ligament Reconstruction: A Systematic Review of Level I Randomized Controlled Trials Comparing Early Postoperative Pain, Opioid Requirements, and Quadriceps Strength.Arthroscopy. 2020 Jul;36(7):1973-1980. doi: 10.1016/j.arthro.2020.03.040. Epub 2020 Apr 18. Arthroscopy. 2020. PMID: 32315764
-
A Comparative Study of Ultrasound-Guided Continuous Adductor Canal Block With Ultrasound-Guided Continuous Femoral Nerve Block in Unilateral Total Knee Arthroplasty for Limb Mobilization and Analgesic Efficacy.Cureus. 2022 Mar 6;14(3):e22904. doi: 10.7759/cureus.22904. eCollection 2022 Mar. Cureus. 2022. PMID: 35265438 Free PMC article.
-
[Clinical application of nerve block in early analgesia after anterior cruciate ligament reconstruction].Zhongguo Gu Shang. 2025 Mar 25;38(3):287-92. doi: 10.12200/j.issn.1003-0034.20230354. Zhongguo Gu Shang. 2025. PMID: 40148091 Chinese.
Cited by
-
Surgeon-Administered Anterolateral Geniculate Nerve Block as an Adjunct to Regional Anesthetic for Pain Management Following Anterior Cruciate Ligament Reconstruction.Arthrosc Tech. 2022 Jan 20;11(1):e1-e6. doi: 10.1016/j.eats.2021.08.034. eCollection 2022 Jan. Arthrosc Tech. 2022. PMID: 35127422 Free PMC article.
-
Effects of esketamine combined with ultrasound-guided nerve block on cognitive function in children with lower extremity fractures.Am J Transl Res. 2021 Jul 15;13(7):7976-7982. eCollection 2021. Am J Transl Res. 2021. PMID: 34377278 Free PMC article.
-
Comparison between femoral block and PENG block in femoral neck fractures: A cohort study.PLoS One. 2021 Jun 4;16(6):e0252716. doi: 10.1371/journal.pone.0252716. eCollection 2021. PLoS One. 2021. PMID: 34086782 Free PMC article.
-
Comparing Analgesic Efficacy of a Novel Dual Subsartorial Block Using Two Different Volumes in Patients Undergoing Total Knee Arthroplasty: A Prospective, Double-Blind, Monocentric, Randomised Trial.Cureus. 2021 Dec 17;13(12):e20488. doi: 10.7759/cureus.20488. eCollection 2021 Dec. Cureus. 2021. PMID: 34934599 Free PMC article.
-
Efficacy of Supplemental Ultrasound-Guided Pericapsular Nerve Group (PENG) Block Combined with Lateral Femoral Cutaneous Nerve Block in Patients Receiving Local Infiltration Analgesia after Hip Fracture Surgery: A Prospective Randomized Controlled Trial.Medicina (Kaunas). 2024 Feb 12;60(2):315. doi: 10.3390/medicina60020315. Medicina (Kaunas). 2024. PMID: 38399602 Free PMC article. Clinical Trial.
References
-
- Bollen SR, Scott BW. Rupture of the anterior cruciate ligament – A quiet epidemic? Injury. 1996;27:407–9. - PubMed
-
- American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in perioperative settings: An updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116:248–73. - PubMed
-
- Kandasami M, Kinninmonth AW, Sarungi M, Baines J, Scott NB. Femoral nerve block for total knee replacement – A word of caution. Knee. 2009;16:98–100. - PubMed
-
- Manickam B, Perlas A, Duggan E, Brull R, Chan VW, Ramlogan R. Feasibility and efficacy of USG guided block of saphenous nerve in the adductor canal. RegAnesth Pain Med. 2009;34:578–80. - PubMed
LinkOut - more resources
Full Text Sources
Medical