

Hiatal hernia involving prolapse of the entire stomach into the mediastinum after distal gastrectomy: a case report
- PMID: 30105511
- PMCID: PMC6089854
- DOI: 10.1186/s40792-018-0503-7
Hiatal hernia involving prolapse of the entire stomach into the mediastinum after distal gastrectomy: a case report
Abstract
Background: Prolapse of a small part of the proximal stomach through the hiatus into the mediastinum is relatively common. Hiatal hernia involving the postoperative stomach has been reported previously, but the degree of hernia was not so severe, and hiatal hernia involving the prolapse of the entire stomach following gastrectomy into the mediastinum has never been reported. We describe a very rare case of large hiatal hernia involving the entire postoperative stomach.
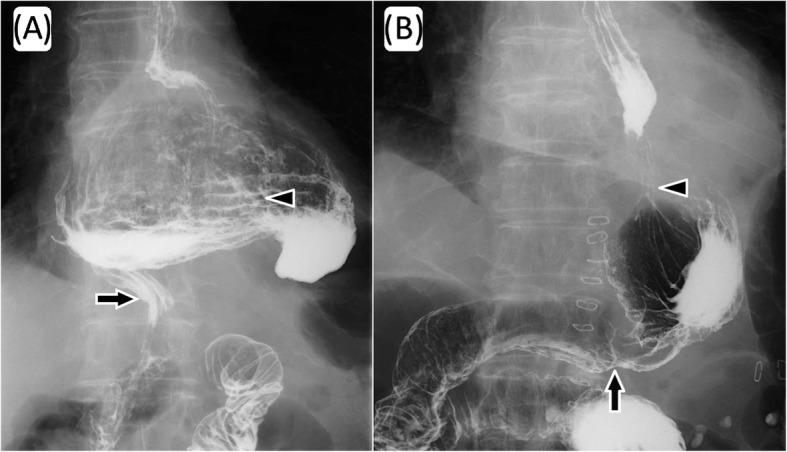
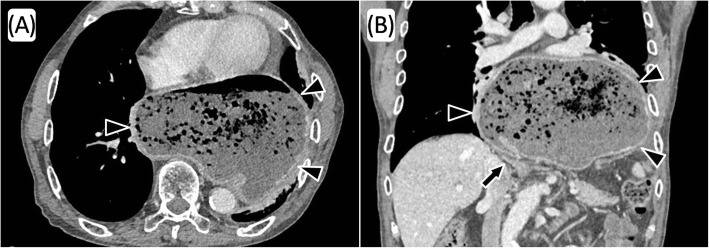
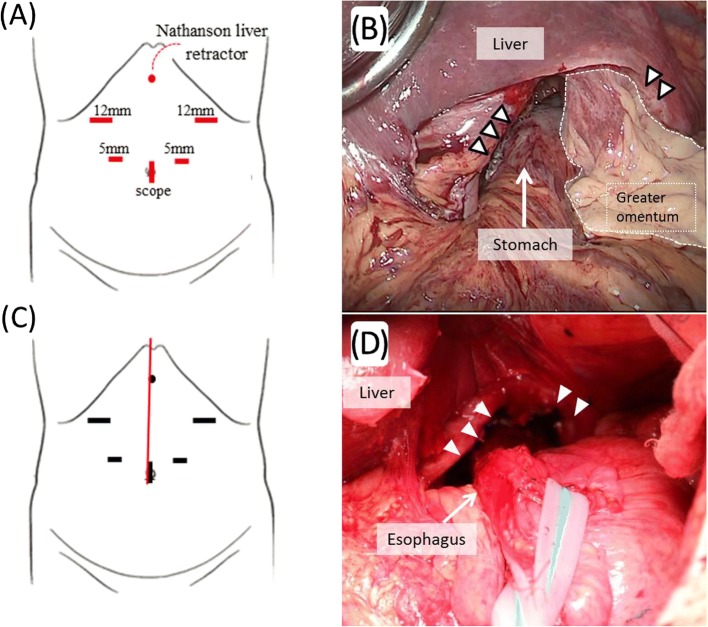
Case presentation: A 79-year-old man with a history of distal gastrectomy for submucosal benign tumor 40 years ago was referred to our hospital because of dysphagia and weight loss. Computed tomography revealed prolapse of the entire postoperative stomach into the mediastinum, and a radical operation was performed. There was a strong adhesion in the hernial sac of the mediastinum, but only little adhesion due to a previous open surgery in the abdominal cavity was present. After the stomach was pulled into the abdominal cavity, suture cruroplasty and Toupet fundoplication without dissection of the short gastric artery were performed. The patient experienced postoperative paralytic ileus, but the rest of the postoperative course was uneventful and the symptom of dysphagia improved.
Conclusions: We presented a very rare large hiatal hernia involving the entire postoperative stomach. Toupet fundoplication preserving the short gastric artery could be one of the optimal surgeries to prevent postoperative regurgitation of the remnant stomach.
Keywords: Fundoplication; Large hiatal hernia; Postgastrectomy.
Conflict of interest statement
Not applicable.
Consent has been obtained in Japanese from the patient to publish clinical data and imaging for the purposes of this case report.
The authors declare that they have no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
