

Randomized Trial of Hypofractionated, Dose-Escalated, Intensity-Modulated Radiation Therapy (IMRT) Versus Conventionally Fractionated IMRT for Localized Prostate Cancer
- PMID: 30106637
- PMCID: PMC6804854
- DOI: 10.1200/JCO.2018.77.9868
Randomized Trial of Hypofractionated, Dose-Escalated, Intensity-Modulated Radiation Therapy (IMRT) Versus Conventionally Fractionated IMRT for Localized Prostate Cancer
Abstract
Purpose: Hypofractionated radiotherapy delivers larger daily doses of radiation and may increase the biologically effective dose delivered to the prostate. We conducted a randomized trial testing the hypothesis that dose-escalated, moderately hypofractionated intensity-modulated radiation therapy (HIMRT) improves prostate cancer control compared with conventionally fractionated IMRT (CIMRT) for men with localized prostate cancer.
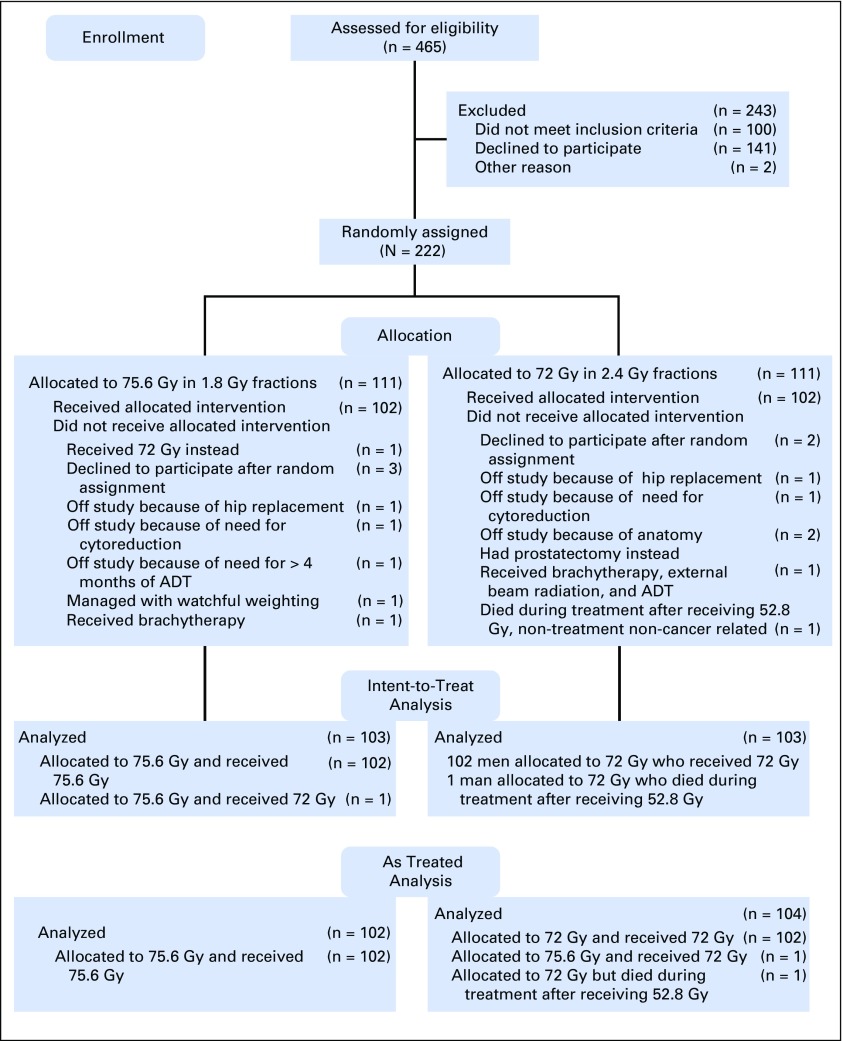
Patients and methods: Men were randomly assigned to 75.6 Gy in 1.8-Gy fractions delivered over 8.4 weeks (CIMRT) or 72 Gy in 2.4 Gy fractions delivered over 6 weeks (HIMRT, biologically equivalent to 85 Gy in 1.8-Gy fractions assuming prostate cancer α-to-β ratio of 1.5). Failure was defined as prostate-specific antigen (PSA) failure (nadir plus 2 ng/mL) or initiation of salvage therapy. Modified Radiation Therapy Oncology Group criteria were used to grade late (≥ 90 days after completion of radiotherapy) GI and genitourinary toxicity.
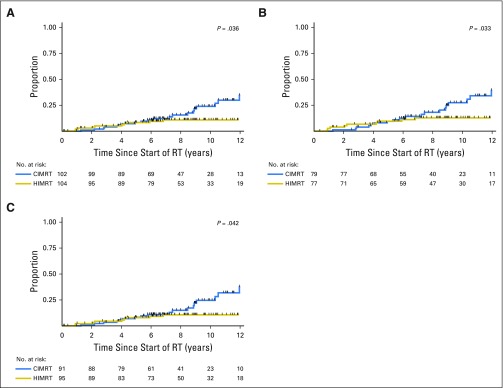
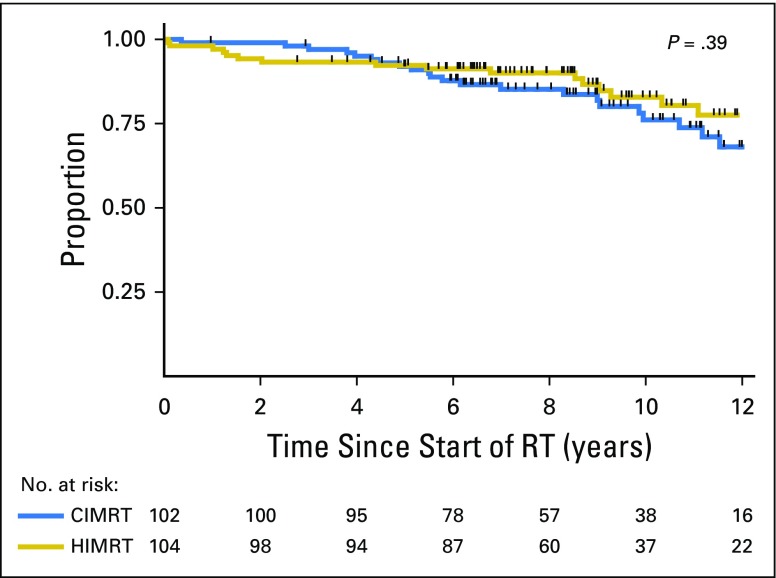
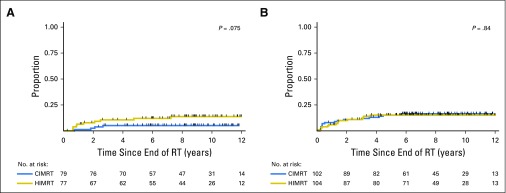
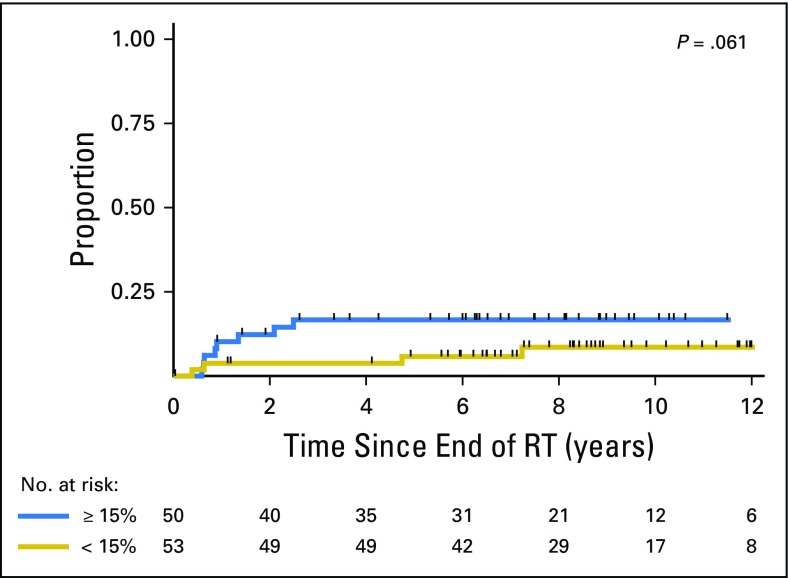
Results: Most of the 206 men (72%) had cT1, Gleason score 6 or 7 (99%), and PSA level ≤ 10 ng/mL (90%) disease. Androgen deprivation therapy was received by 24%. With a median follow-up of 8.5 years, men treated with HIMRT experienced fewer treatment failures (n = 10) than men treated with CIMRT (n = 21; P = .036). The 8-year failure rate was 10.7% (95% CI, 5.8% to 19.1%) with HIMRT and 15.4% (95% CI, 9.1% to 25.4%) with CIMRT. There was no difference in overall survival ( P = .39). There was a nonsignificant increase in late grade 2 or 3 GI toxicity with HIMRT (8-year 5.0% v 12.6%; P = .08). However, GI toxicity was only 8.6% when rectal volume receiving 65 Gy of HIMRT was ≤ 15%. Late genitourinary toxicity was similar ( P = .84). There was no grade 4 toxicity.
Conclusion: The results of this randomized trial demonstrate superior cancer control for men with localized prostate cancer who receive dose-escalated moderately hypofractionation radiotherapy while shortening treatment duration.
Figures
Comment in
-
Prostate Cancer Radiotherapy: An Evolving Paradigm.J Clin Oncol. 2018 Oct 10;36(29):2909-2913. doi: 10.1200/JCO.2018.79.3257. Epub 2018 Aug 23. J Clin Oncol. 2018. PMID: 30138084
-
Re: Randomized Trial of Hypofractionated, Dose-Escalated, Intensity-Modulated Radiation Therapy (IMRT) versus Conventionally Fractionated IMRT for Localized Prostate Cancer.J Urol. 2019 May;201(5):859. doi: 10.1097/JU.0000000000000169. J Urol. 2019. PMID: 30747871 No abstract available.
References
-
- Beckendorf V, Guerif S, Le Prisé E, et al. 70 Gy versus 80 Gy in localized prostate cancer: 5-Year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys. 2011;80:1056–1063. - PubMed
-
- Dearnaley DP, Jovic G, Syndikus I, et al. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: Long-term results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2014;15:464–473. - PubMed
-
- Heemsbergen WD, Al-Mamgani A, Slot A, et al. Long-term results of the Dutch randomized prostate cancer trial: impact of dose-escalation on local, biochemical, clinical failure, and survival. Radiother Oncol. 2014;110:104–109. - PubMed
-
- Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:67–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
