

Complexity in disease management: A linked data analysis of multimorbidity in Aboriginal and non-Aboriginal patients hospitalised with atherothrombotic disease in Western Australia
- PMID: 30106971
- PMCID: PMC6091927
- DOI: 10.1371/journal.pone.0201496
Complexity in disease management: A linked data analysis of multimorbidity in Aboriginal and non-Aboriginal patients hospitalised with atherothrombotic disease in Western Australia
Abstract
Background: Hospitalisation for atherothrombotic disease (ATD) is expected to rise in coming decades. However, increasingly, associated comorbidities impose challenges in managing patients and deciding appropriate secondary prevention. We investigated the prevalence and pattern of multimorbidity (presence of two or more chronic conditions) in Aboriginal and non-Aboriginal Western Australian residents with ATDs.
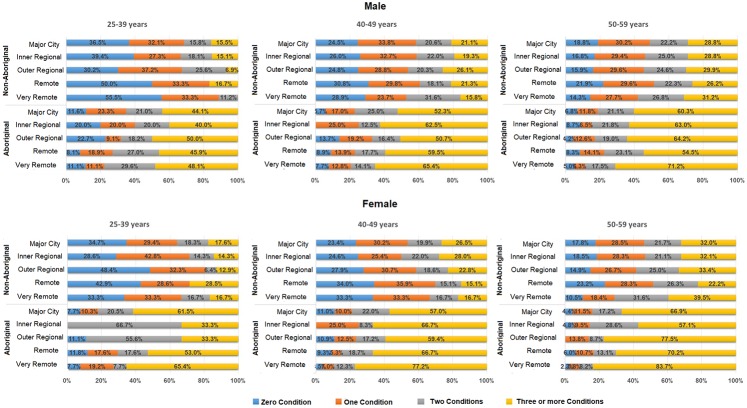
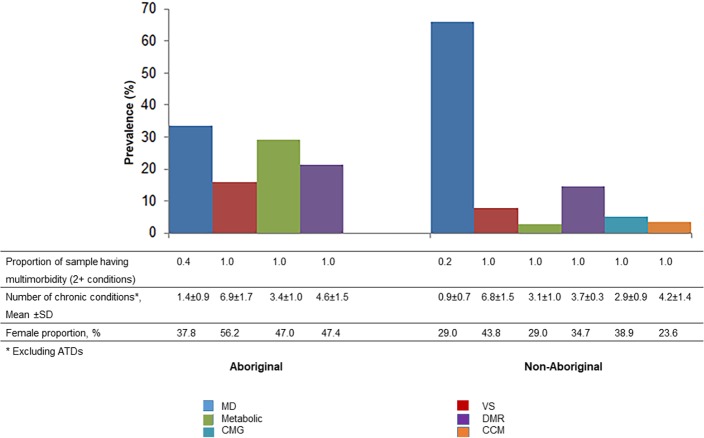
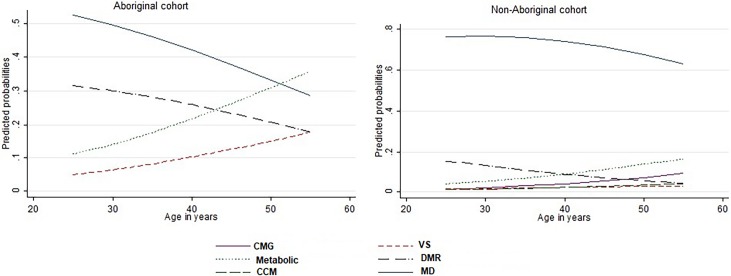
Methods and findings: We used population-based de-identified linked administrative health data from 1 January 2000 to 30 June 2014 to identify a cohort of patients aged 25-59 years admitted to Western Australian hospitals with a discharge diagnosis of ATD. The prevalence of common chronic diseases in these patients was estimated and the patterns of comorbidities and multimorbidities empirically explored using two different approaches: identification of the most commonly occurring pairs and triplets of comorbid diseases, and through latent class analysis (LCA). Half of the cohort had multimorbidity, although this was much higher in Aboriginal people (Aboriginal: 79.2% vs. non-Aboriginal: 39.3%). Only a quarter were without any documented comorbidities. Hypertension, diabetes, alcohol abuse disorders and acid peptic diseases were the leading comorbidities in the major comorbid combinations across both Aboriginal and non-Aboriginal cohorts. The LCA identified four and six distinct clinically meaningful classes of multimorbidity for Aboriginal and non-Aboriginal patients, respectively. Out of the six groups in non-Aboriginal patients, four were similar to the groups identified in Aboriginal patients. The largest proportion of patients (33% in Aboriginal and 66% in non-Aboriginal) was assigned to the "minimally diseased" (or relatively healthy) group, with most patients having less than two conditions. Other groups showed variability in degree and pattern of multimorbidity.
Conclusion: Multimorbidity is common in ATD patients and the comorbidities tend to interact and cluster together. Physicians need to consider these in their clinical practice. Different treatment and secondary prevention strategies are likely to be useful for management in these cluster groups.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Multimorbidity among Aboriginal people in New South Wales contributes significantly to their higher mortality.Med J Aust. 2018 Jun 2;209(1):19-23. doi: 10.5694/mja17.00878. Med J Aust. 2018. PMID: 29954311
-
Prevalence and patterns of multimorbidity in Australian baby boomers: the Busselton healthy ageing study.BMC Public Health. 2021 Aug 11;21(1):1539. doi: 10.1186/s12889-021-11578-y. BMC Public Health. 2021. PMID: 34380465 Free PMC article.
-
Multimorbidity in a marginalised, street-health Australian population: a retrospective cohort study.BMJ Open. 2014 Aug 19;4(8):e005461. doi: 10.1136/bmjopen-2014-005461. BMJ Open. 2014. PMID: 25138806 Free PMC article.
-
Multimorbidity disease clusters in Aboriginal and non-Aboriginal Caucasian populations in Canada.Chronic Dis Inj Can. 2014 Nov;34(4):218-25. Chronic Dis Inj Can. 2014. PMID: 25408181 English, French.
-
Interventions for improving outcomes in patients with multimorbidity in primary care and community settings.Cochrane Database Syst Rev. 2021 Jan 15;1(1):CD006560. doi: 10.1002/14651858.CD006560.pub4. Cochrane Database Syst Rev. 2021. PMID: 33448337 Free PMC article.
Cited by
-
Use of latent class analysis to identify multimorbidity patterns and associated factors in Korean adults aged 50 years and older.PLoS One. 2019 Nov 13;14(11):e0216259. doi: 10.1371/journal.pone.0216259. eCollection 2019. PLoS One. 2019. PMID: 31721778 Free PMC article.
-
Let's CHAT (community health approaches to) dementia in Aboriginal and Torres Strait Islander communities: protocol for a stepped wedge cluster randomised controlled trial.BMC Health Serv Res. 2020 Mar 12;20(1):208. doi: 10.1186/s12913-020-4985-1. BMC Health Serv Res. 2020. PMID: 32164678 Free PMC article. Clinical Trial.
-
Detection of cognitive impairment, dementia and associated risk factors among Aboriginal and Torres Strait Islander peoples: Retrospective baseline audit results from a stepped-wedge cluster-randomised controlled trial.Australas J Ageing. 2025 Mar;44(1):e70007. doi: 10.1111/ajag.70007. Australas J Ageing. 2025. PMID: 40044610 Free PMC article. Clinical Trial.
-
Challenges in Managing Acute Cardiovascular Diseases and Follow Up Care in Rural Areas: A Narrative Review.Int J Environ Res Public Health. 2019 Dec 15;16(24):5126. doi: 10.3390/ijerph16245126. Int J Environ Res Public Health. 2019. PMID: 31847490 Free PMC article. Review.
-
Considerations in Planning Physical Activity for Older Adults in Hot Climates: A Narrative Review.Int J Environ Res Public Health. 2021 Feb 2;18(3):1331. doi: 10.3390/ijerph18031331. Int J Environ Res Public Health. 2021. PMID: 33540584 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
