

Controlled attenuation parameter does not predict hepatic decompensation in patients with advanced chronic liver disease
- PMID: 30107095
- PMCID: PMC6585636
- DOI: 10.1111/liv.13943
Controlled attenuation parameter does not predict hepatic decompensation in patients with advanced chronic liver disease
Abstract
Background & aims: Assessment of hepatic steatosis by transient elastography (TE)-based controlled attenuation parameter (CAP) might predict hepatic decompensation. Therefore, we aimed to evaluate the prognostic value of CAP in patients with compensated advanced chronic liver disease (cACLD) and decompensated cirrhosis (DC).
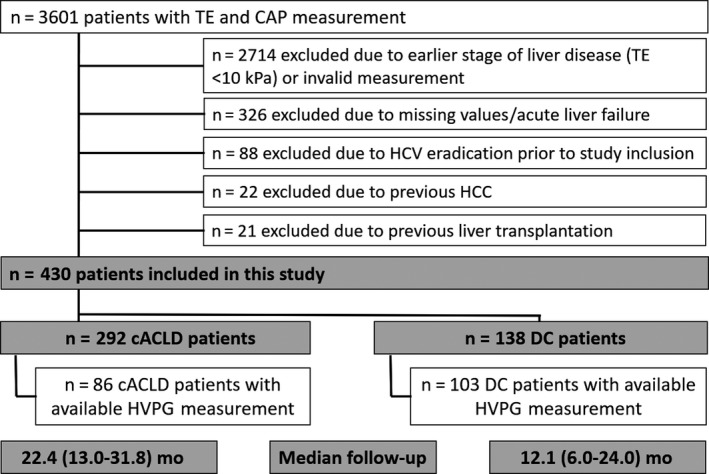
Methods: A total of 430 patients who underwent TE (liver stiffness ≥10 kPa) and CAP measurements were included in this retrospective analysis. Half of patients (n = 189) underwent simultaneous HVPG measurement. In cACLD patients, first hepatic decompensation was defined by new onset of ascites, hepatic encephalopathy or variceal bleeding. In patients with DC, the following events were considered as further hepatic decompensation: requirement of paracentesis, admission for/development of grade 3/4 hepatic encephalopathy, variceal (re-)bleeding or liver-related death.
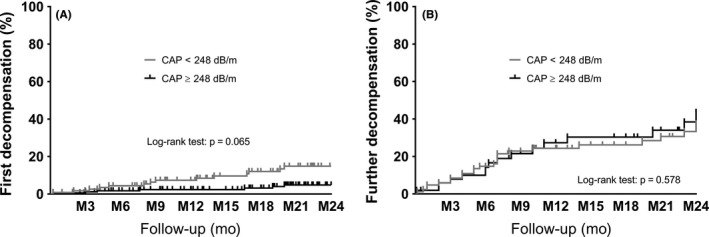
Results: First hepatic decompensation occurred in 25 of 292 (9%) cACLD patients, while 46 of 138 (33%) DC patients developed further hepatic decompensation during a median follow-up of 22 and 12 months respectively. CAP was not predictive of first (cACLD; per 10 dB/m; hazard ratio [HR]: 0.97, 95% confidence interval [95% CI]: 0.91-1.03, P = 0.321) or further hepatic decompensation (DC; HR: 0.99, 95% CI: 0.94-1.03, P = 0.554) in adjusted analysis. Using the well-established CAP cut-off of ≥248 dB/m for hepatic steatosis, the incidence of first (cACLD; P = 0.065) and further hepatic decompensation (DC; P = 0.578) was similar in patients with hepatic steatosis or without. Serum albumin levels (per mg/dL; HR: 0.83, 95% CI: 0.77-0.89, P < 0.001) and MELD-Na (per point; HR: 1.15, 95% CI: 1.04-1.28, P = 0.006) in cACLD and MELD-Na (per point; HR: 1.12, 95% CI: 1.05-1.19, P < 0.0001) in DC patients were the only parameters independently associated with first and further hepatic decompensation, respectively.
Conclusion: Controlled attenuation parameter does not predict the development of first (cACLD)/further (DC) hepatic decompensation, while serum albumin levels and MELD-Na are of prognostic value.
Keywords: compensated advanced chronic liver disease; controlled attenuation parameter; decompensated cirrhosis; hepatic decompensation.
© 2018 The Authors. Liver International Published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have nothing to disclose regarding this study.
Figures
Similar articles
-
Hepatic venous pressure gradient predicts risk of hepatic decompensation and liver-related mortality in patients with MASLD.J Hepatol. 2024 Nov;81(5):827-836. doi: 10.1016/j.jhep.2024.05.033. Epub 2024 May 31. J Hepatol. 2024. PMID: 38823501
-
Measurement of Spleen Stiffness With Acoustic Radiation Force Impulse Imaging Predicts Mortality and Hepatic Decompensation in Patients With Liver Cirrhosis.Clin Gastroenterol Hepatol. 2017 Nov;15(11):1782-1790.e4. doi: 10.1016/j.cgh.2016.10.041. Epub 2016 Dec 23. Clin Gastroenterol Hepatol. 2017. PMID: 28017842
-
Using liver stiffness to predict and monitor the risk of decompensation and mortality in patients with alcohol-related liver disease.J Hepatol. 2024 Jul;81(1):23-32. doi: 10.1016/j.jhep.2024.02.019. Epub 2024 Feb 28. J Hepatol. 2024. PMID: 38428644
-
A systematic review of noninvasive laboratory indices and elastography to predict hepatic decompensation.Hepatol Commun. 2025 Mar 24;9(4):e0675. doi: 10.1097/HC9.0000000000000675. eCollection 2025 Apr 1. Hepatol Commun. 2025. PMID: 40131017 Free PMC article.
-
Preventing the progression of cirrhosis to decompensation and death.Nat Rev Gastroenterol Hepatol. 2025 Apr;22(4):265-280. doi: 10.1038/s41575-024-01031-x. Epub 2025 Jan 27. Nat Rev Gastroenterol Hepatol. 2025. PMID: 39870944 Review.
Cited by
-
Distinct prognostic value of different portal hypertension-associated features in patients with primary biliary cholangitis.J Gastroenterol. 2022 Feb;57(2):99-110. doi: 10.1007/s00535-021-01839-3. Epub 2021 Dec 11. J Gastroenterol. 2022. PMID: 34893924 Free PMC article.
-
Novel reliability criteria for controlled attenuation parameter assessments for non-invasive evaluation of hepatic steatosis.United European Gastroenterol J. 2020 Apr;8(3):321-331. doi: 10.1177/2050640619900820. Epub 2020 Jan 17. United European Gastroenterol J. 2020. PMID: 32213023 Free PMC article.
-
Serum levels of gamma-glutamyltransferase predict outcome in heart failure with preserved ejection fraction.Sci Rep. 2019 Dec 6;9(1):18541. doi: 10.1038/s41598-019-55116-8. Sci Rep. 2019. PMID: 31811258 Free PMC article.
-
Exploring Opportunities to Enhance the Screening and Surveillance of Hepatocellular Carcinoma in Non-Alcoholic Fatty Liver Disease (NAFLD) through Risk Stratification Algorithms Incorporating Ultrasound Elastography.Cancers (Basel). 2023 Aug 14;15(16):4097. doi: 10.3390/cancers15164097. Cancers (Basel). 2023. PMID: 37627125 Free PMC article. Review.
-
MRI-defined sarcopenia predicts mortality in patients with chronic liver disease.Liver Int. 2020 Nov;40(11):2797-2807. doi: 10.1111/liv.14648. Liver Int. 2020. PMID: 32816394 Free PMC article.
References
-
- Villanueva C, Albillos A, Genesca J, et al. Development of hyperdynamic circulation and response to eta‐blockers in compensated cirrhosis with portal hypertension. Hepatology. 2016;63(1):197‐206. - PubMed
-
- Reiberger T, Mandorfer M. Beta adrenergic blockade and decompensated cirrhosis. J Hepatol. 2017;66(4):849‐859. - PubMed
-
- Scheiner B, Parada‐Rodriguez D, Bucsics T, et al. Non‐selective beta‐blocker treatment does not impact on kidney function in cirrhotic patients with varices. Scand J Gastroenterol. 2017;52(9):1008‐1015. - PubMed
-
- Francque S, Wamutu S, Chatterjee S, et al. Non‐alcoholic steatohepatitis induces non‐fibrosis‐related portal hypertension associated with splanchnic vasodilation and signs of a hyperdynamic circulation in vitro and in vivo in a rat model. Liver Int. 2010;30(3):365‐375. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
