

Undertriage of major trauma patients at a university hospital: a retrospective cohort study
- PMID: 30107855
- PMCID: PMC6092794
- DOI: 10.1186/s13049-018-0524-z
Undertriage of major trauma patients at a university hospital: a retrospective cohort study
Abstract
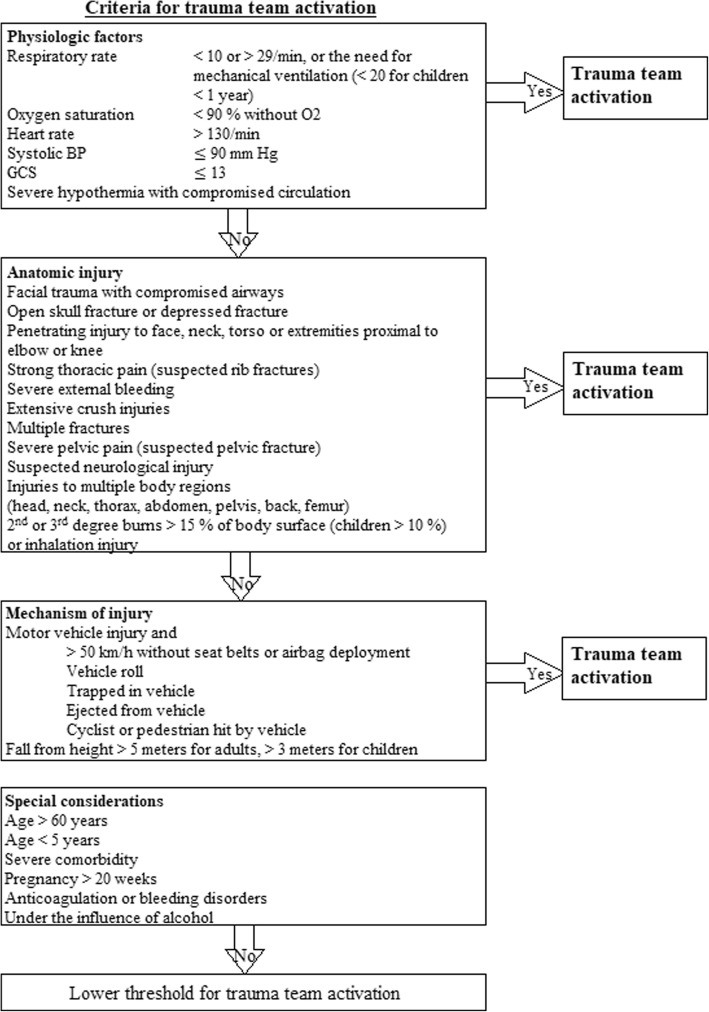
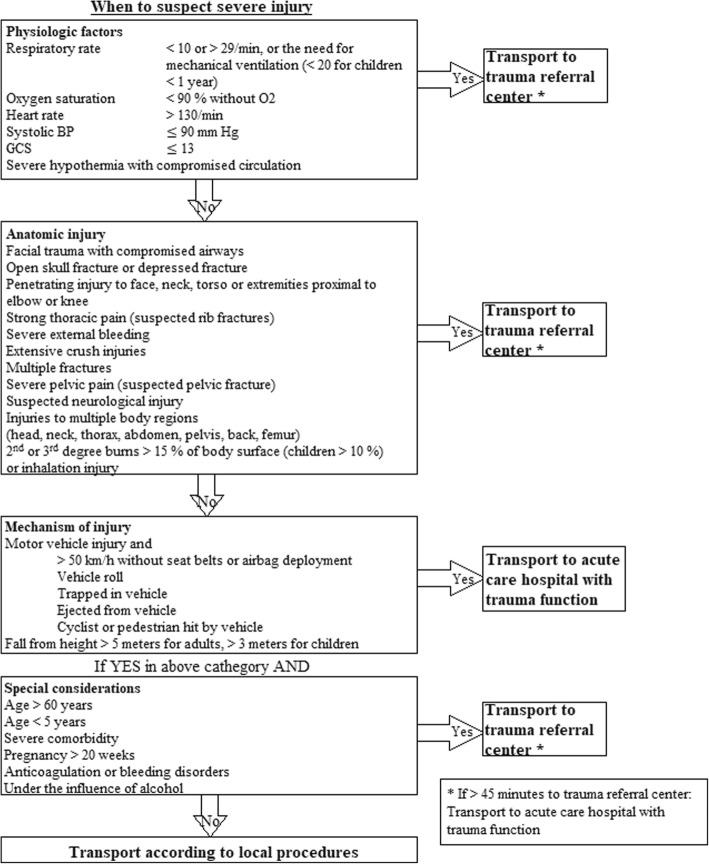
Background: Studies show increased mortality among severely injured patients not met by trauma team. Proper triage is important to ensure that all severely injured patients receive vital trauma care. In 2017 a new national trauma plan was implemented in Norway, which recommended the use of a modified version of "Guidelines for Field Triage of Injured Patients" to identify severely injured patients.
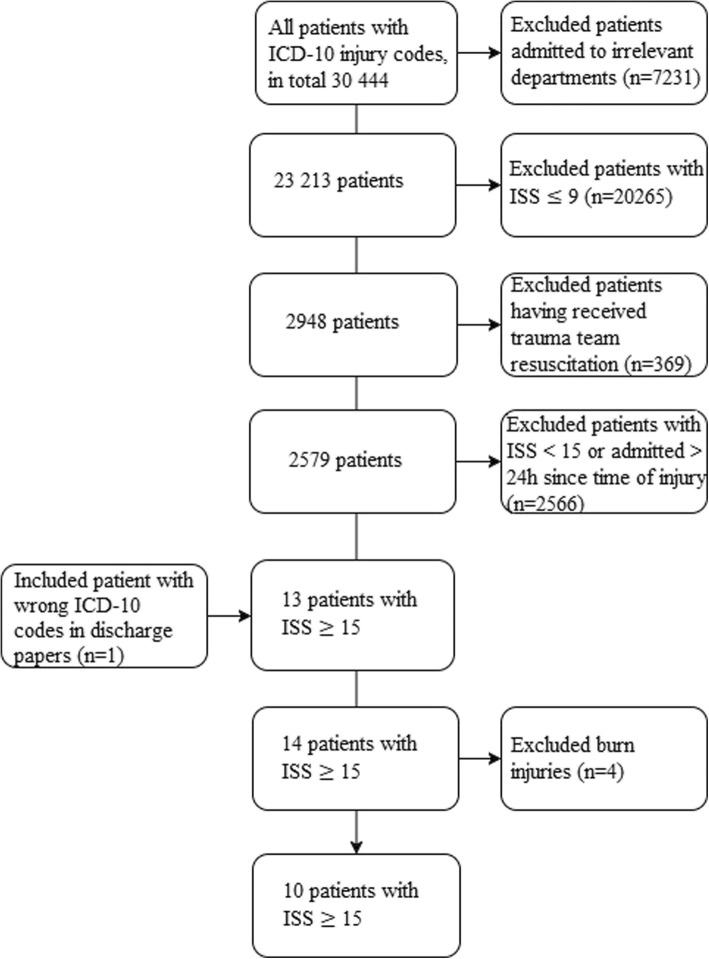
Methods: A retrospective study of 30,444 patients admitted to Haukeland University Hospital in 2013, with ICD-10 injury codes upon discharge. The exclusion criteria were department affiliation considered irrelevant when identifying trauma, patients with injuries that resulted in Injury Severity Score < 15, patients that did receive trauma team, and patients admitted > 24 h after time of injury. Information from patient records of every severely injured patient admitted in 2013 was obtained in order to investigate the sensitivity of the new guidelines.
Results: Trauma team activation was performed in 369 admissions and 85 patients were identified as major trauma. Ten severely injured patients did not receive trauma team resuscitation, resulting in an undertriage of 10.5%. Nine out of ten patients were men, median age 54 years. Five patients were 60 years or older. All of the undertriaged patients experienced fall from low height (< 4 m). Traumatic brain injury was seen in six patients. Six patients had a Glasgow Coma Scale score ≤ 13. The new trauma activation guidelines had a sensitivity of 95.0% in our 2013 trauma population. The degree of undertriage could have been reduced to 4.0% had the guidelines been implemented and correctly applied.
Conclusions: The rate of undertriage at Haukeland University Hospital in 2013 was above the recommendations of less than 5%. Use of the new trauma guidelines showed increased triage precision in the present trauma population.
Keywords: American College of Surgeons, Committee on trauma; Guidelines for Field Triage of Injured Patients; Haukeland University Hospital; National Trauma Plan; Norway; Trauma; Trauma team; Undertriage.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Noncompliance with American College of Surgeons Committee on Trauma recommended criteria for full trauma team activation is associated with undertriage deaths.J Trauma Acute Care Surg. 2018 Feb;84(2):287-294. doi: 10.1097/TA.0000000000001745. J Trauma Acute Care Surg. 2018. PMID: 29360717
-
Precision of field triage in patients brought to a trauma centre after introducing trauma team activation guidelines.Scand J Trauma Resusc Emerg Med. 2009 Jan 9;17:1. doi: 10.1186/1757-7241-17-1. Scand J Trauma Resusc Emerg Med. 2009. PMID: 19134177 Free PMC article.
-
Accuracy of the field triage protocol in selecting severely injured patients after high energy trauma.Injury. 2014 May;45(5):869-73. doi: 10.1016/j.injury.2013.12.010. Epub 2014 Jan 8. Injury. 2014. PMID: 24472800
-
Accuracy of prehospital triage protocols in selecting severely injured patients: A systematic review.J Trauma Acute Care Surg. 2017 Aug;83(2):328-339. doi: 10.1097/TA.0000000000001516. J Trauma Acute Care Surg. 2017. PMID: 28452898
-
Field-Triage, Hospital-Triage and Triage-Assessment: A Literature Review of the Current Phases of Adult Trauma Triage.J Trauma Acute Care Surg. 2021 Jun 1;90(6):e138-e145. doi: 10.1097/TA.0000000000003125. J Trauma Acute Care Surg. 2021. PMID: 33605709 Review.
Cited by
-
Evaluation of Prehospital Undertriage in Relation to Trauma Team Activation-Results from a Prospective Study in 12 Level one German Trauma Centers.J Clin Med. 2024 Mar 16;13(6):1714. doi: 10.3390/jcm13061714. J Clin Med. 2024. PMID: 38541939 Free PMC article.
-
Delayed Neurosurgical Intervention in Traumatic Brain Injury Patients Referred From Primary Hospitals Is Not Associated With an Unfavorable Outcome.Front Neurol. 2021 Jan 13;11:610192. doi: 10.3389/fneur.2020.610192. eCollection 2020. Front Neurol. 2021. PMID: 33519689 Free PMC article.
-
Exploring the effectiveness of artificial intelligence, machine learning and deep learning in trauma triage: A systematic review and meta-analysis.Digit Health. 2023 Oct 9;9:20552076231205736. doi: 10.1177/20552076231205736. eCollection 2023 Jan-Dec. Digit Health. 2023. PMID: 37822960 Free PMC article. Review.
-
Differences in characteristics between patients ≥ 65 and < 65 years of age with orthopaedic injuries after severe trauma.Scand J Trauma Resusc Emerg Med. 2022 Sep 24;30(1):51. doi: 10.1186/s13049-022-01038-w. Scand J Trauma Resusc Emerg Med. 2022. PMID: 36153545 Free PMC article.
-
'Board' out of my skull: penetrating skull fracture from a surfboard nose.BMJ Case Rep. 2018 Dec 3;11(1):bcr2018227678. doi: 10.1136/bcr-2018-227678. BMJ Case Rep. 2018. PMID: 30567182 Free PMC article. No abstract available.
References
-
- McDermott FT, Cordner SM. Victoria's trauma care system: national implications for quality improvement. Med J Aust. 2008;189(10):540–542. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
