

Pilot Study of the Effects of High-Protein Meals During Hemodialysis on Intradialytic Hypotension in Patients Undergoing Maintenance Hemodialysis
- PMID: 30107974
- PMCID: PMC6370529
- DOI: 10.1053/j.jrn.2018.06.002
Pilot Study of the Effects of High-Protein Meals During Hemodialysis on Intradialytic Hypotension in Patients Undergoing Maintenance Hemodialysis
Abstract
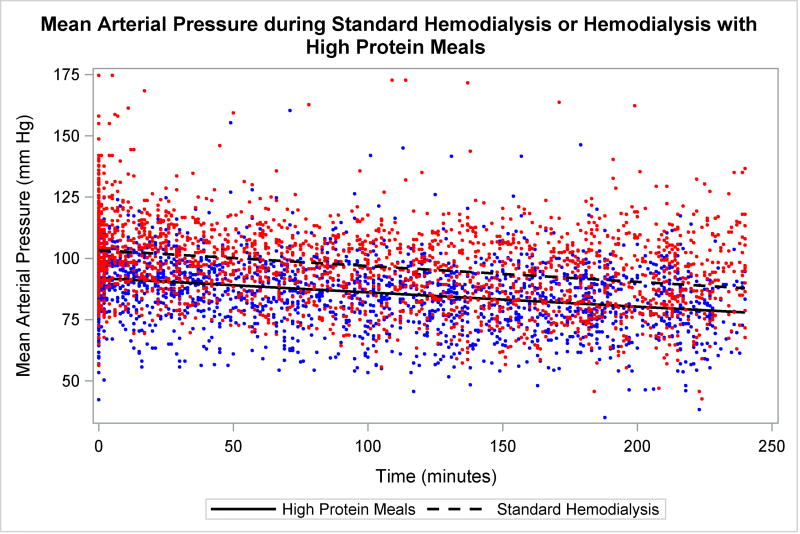
Objective: Patients undergoing hemodialysis (HD) have high protein and energy requirements, and protein-energy wasting is common and associated with poor outcomes. Eating during dialysis may improve nutritional status by counteracting the catabolic effects of HD treatment; but eating during HD may be discouraged because of concerns of postprandial hypotension. However, little data are available to support this practice. In this study, we hypothesized that high-protein meals during HD do not lead to symptomatic intradialytic hypotension events.
Design: A 9-week, nonrandomized, parallel-arm study.
Setting: A single in-center HD clinic.
Subjects: Eighteen patients undergoing HD from 2 shifts completed the study. Patients were aged 62 ± 16 years with dialysis vintage of 3.4 ± 2.6 years.
Intervention: Patients in the intervention group (n = 9) undergoing HD received meals of ∼30 g protein and ∼1/3 daily recommended intakes of sodium, potassium, phosphorus, and fluid during dialysis for 25 consecutive HD sessions. The control group (n = 9) completed all aspects of the study including a visit by study personnel but were not given meals. The 25 consecutive sessions before the start of the intervention/control phase were used as a baseline comparison for each patient.
Main outcome measure: Symptomatic hypotension event frequency.
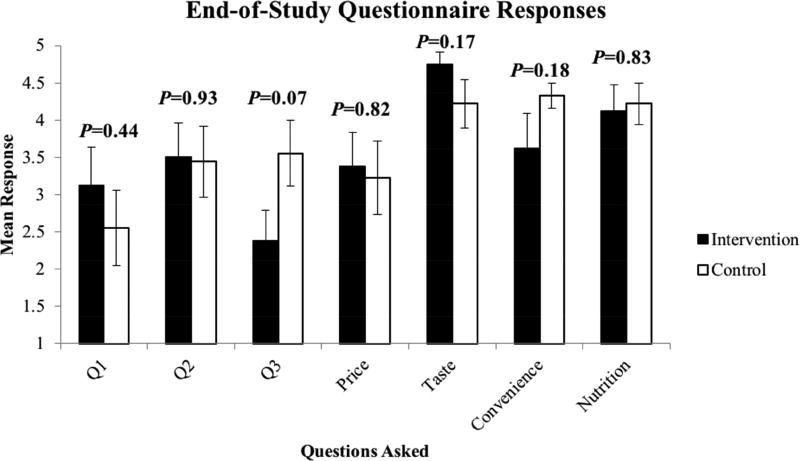
Results: In the intervention arm, there were 19 symptomatic hypotension events in 5 patients prestudy and 18 events in 6 patients during the study. In the control arm, there were 16 events in 7 patients prestudy and 13 events in 7 patients during the study. Change in the frequency of symptomatic hypotension events from prestudy to during study was not different between groups (P = .71). There was no effect of meals on nutritional status, but patients reported positive attitudes toward receiving meals during dialysis.
Conclusion: High-protein meals during HD did not increase symptomatic hypotension events. Larger, longer term studies are needed to confirm these results and evaluate whether high-protein meals on dialysis benefit nutritional status and clinical outcomes.
Copyright © 2018 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
High Animal and Vegetarian Protein Intake in Hemodialysis Patients.J Ren Nutr. 2019 May;29(3):248. doi: 10.1053/j.jrn.2018.08.012. Epub 2018 Oct 8. J Ren Nutr. 2019. PMID: 30309782 No abstract available.
References
-
- United States Renal Data System. 2015 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2015.
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–266. - PubMed
-
- Iliescu EA, Coo H, McMurray MH, et al. Quality of sleep and health-related quality of life in haemodialysis patients. Nephrol Dial Transplant. 2003;18(1):126–132. - PubMed
-
- Kalantar-Zadeh K, Fouque D. Nutritional Management of Chronic Kidney Disease. N Engl J Med. 2017;377(18):1765–1776. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
