

Exercise-induced bronchoconstriction: prevalence, pathophysiology, patient impact, diagnosis and management
- PMID: 30108224
- PMCID: PMC6092370
- DOI: 10.1038/s41533-018-0098-2
Exercise-induced bronchoconstriction: prevalence, pathophysiology, patient impact, diagnosis and management
Abstract
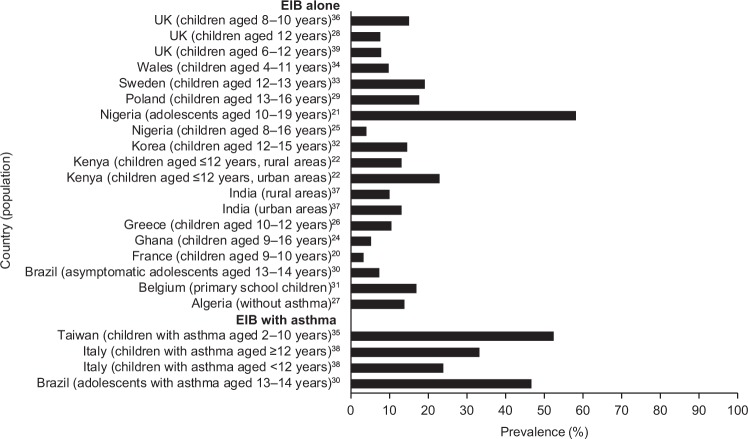
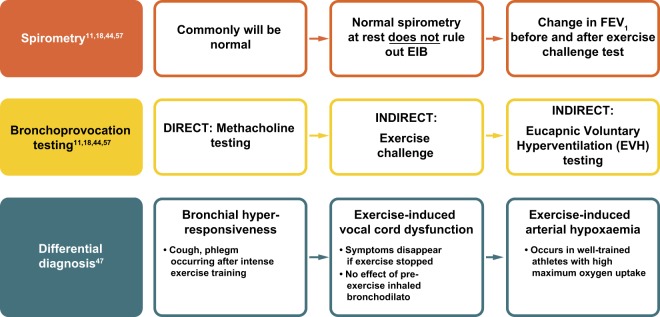
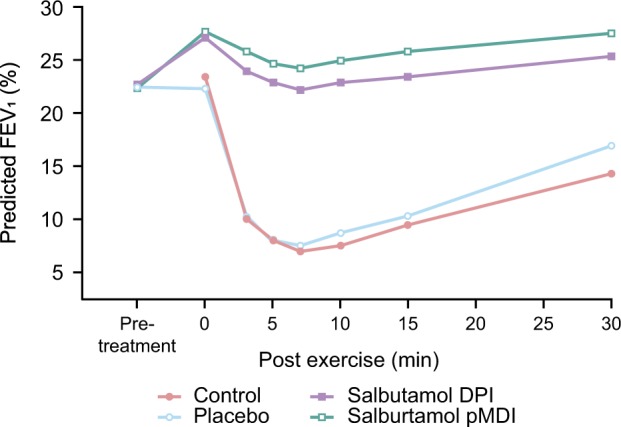
Exercise-induced bronchoconstriction (EIB) can occur in individuals with and without asthma, and is prevalent among athletes of all levels. In patients with asthma, symptoms of EIB significantly increase the proportion reporting feelings of fearfulness, frustration, isolation, depression and embarrassment compared with those without symptoms. EIB can also prevent patients with asthma from participating in exercise and negatively impact their quality of life. Diagnosis of EIB is based on symptoms and spirometry or bronchial provocation tests; owing to low awareness of EIB and lack of simple, standardised diagnostic methods, under-diagnosis and mis-diagnosis of EIB are common. To improve the rates of diagnosis of EIB in primary care, validated and widely accepted symptom-based questionnaires are needed that can accurately replicate the current diagnostic standards (forced expiratory volume in 1 s reductions observed following exercise or bronchoprovocation challenge) in patients with and without asthma. In patients without asthma, EIB can be managed by various non-pharmacological methods and the use of pre-exercise short-acting β2-agonists (SABAs). In patients with asthma, EIB is often associated with poor asthma control but can also occur in individuals who have good control when not exercising. Inhaled corticosteroids are recommended when asthma control is suboptimal; however, pre-exercise SABAs are also widely used and are recommended as the first-line therapy. This review describes the burden, key features, diagnosis and current treatment approaches for EIB in patients with and without asthma and serves as a call to action for family physicians to be aware of EIB and consider it as a potential diagnosis.
Conflict of interest statement
B.A., A.M. and N.B. are employees of GSK and hold stocks or shares in the company.
Figures
References
-
- McNeill RS, Nairn JR, Millar JS, Ingram CG. Exercise-induced asthma. Q. J. Med. 1966;35:55–67. - PubMed
-
- Fisher HK, Holton P, Buxton RS, Nadel JA. Resistance to breathing during exercise-induced asthma attacks. Am. Rev. Respir. Dis. 1970;101:885–896. - PubMed
-
- Bierman EW, Kawabori I, Pierson WE. Incidence of exercise-induced asthma in children. Pediatrics. 1975;56:847–850. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
