

A " Blood Relationship" Between the Overlooked Minimum Lactate Equivalent and Maximal Lactate Steady State in Trained Runners. Back to the Old Days?
- PMID: 30108519
- PMCID: PMC6079548
- DOI: 10.3389/fphys.2018.01034
A " Blood Relationship" Between the Overlooked Minimum Lactate Equivalent and Maximal Lactate Steady State in Trained Runners. Back to the Old Days?
Abstract
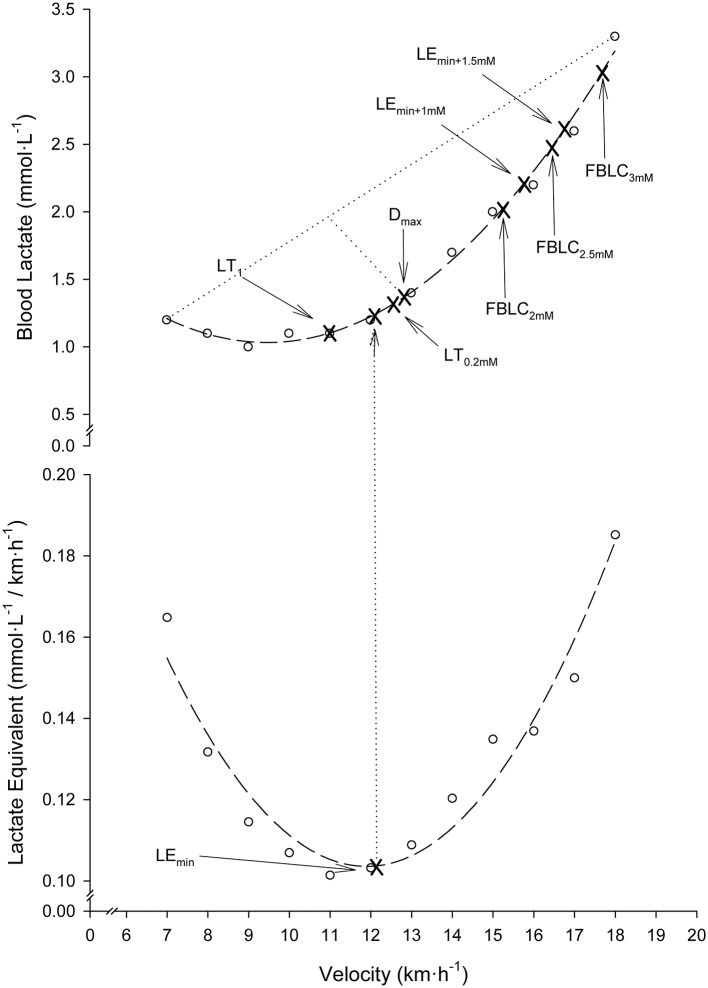
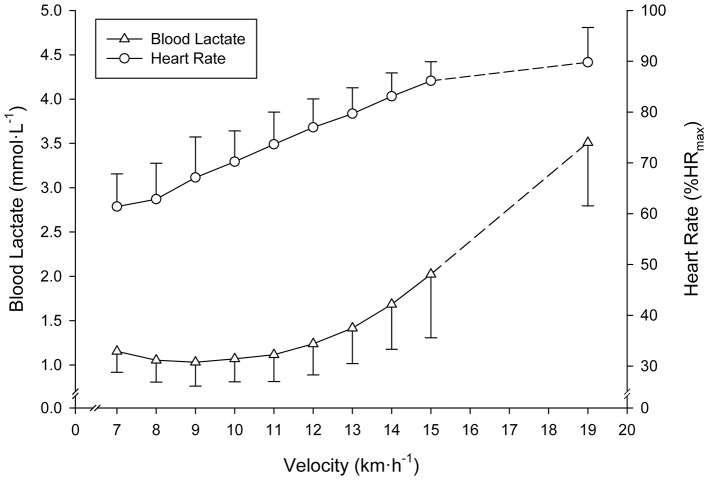
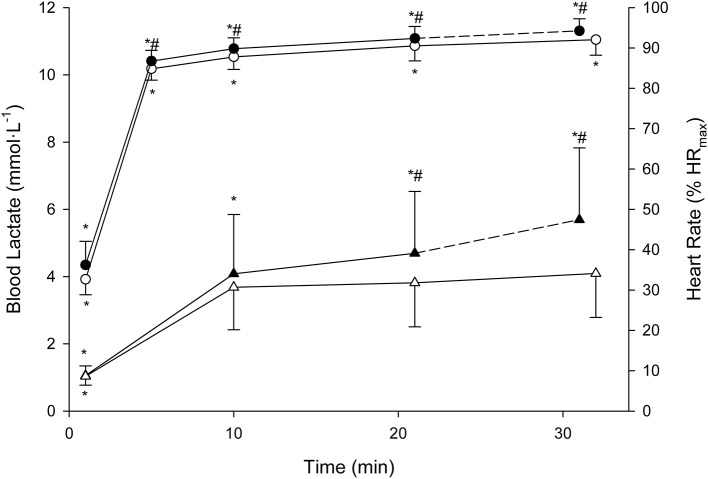
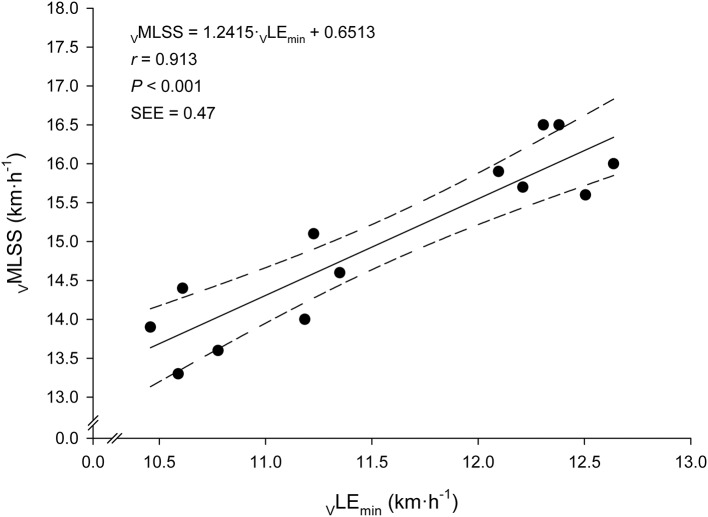
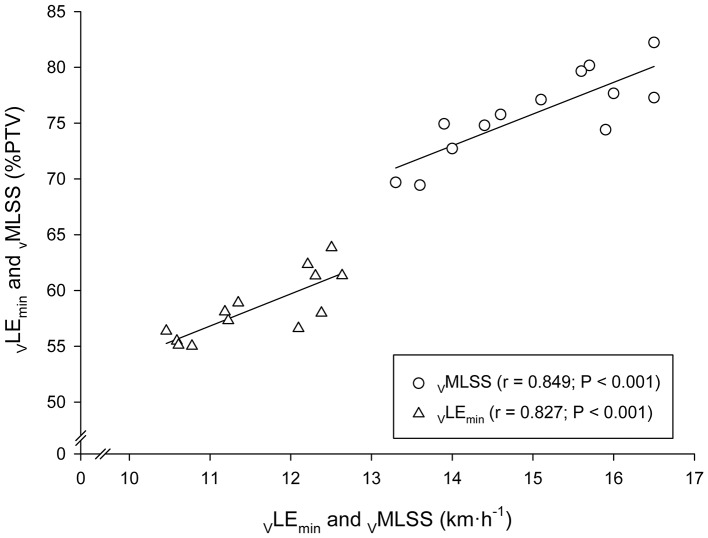
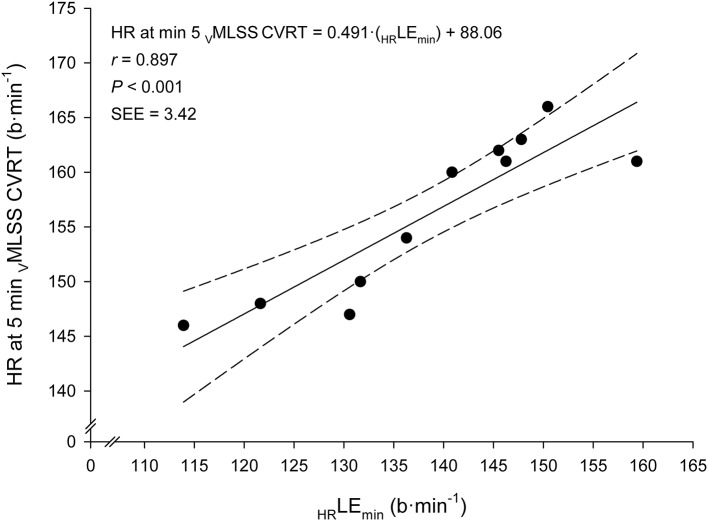
Maximal Lactate Steady State (MLSS) and Lactate Threshold (LT) are physiologically-related and fundamental concepts within the sports and exercise sciences. Literature supporting their relationship, however, is scarce. Among the recognized LTs, we were particularly interested in the disused "Minimum Lactate Equivalent" (LEmin), first described in the early 1980s. We hypothesized that velocity at LT, conceptually comprehended as in the old days (LEmin), could predict velocity at MLSS (VMLSS) more accurate than some other blood lactate-related thresholds (BLRTs) routinely used nowadays by many sport science practitioners. Thirteen male endurance-trained [VMLSS 15.0 ± 1.1 km·h-1; maximal oxygen uptake ( ) 67.6 ± 4.1 ml·kg-1·min-1] homogeneous (coefficient of variation: ≈7%) runners conducted 1) a submaximal discontinuous incremental running test to determine several BLRTs followed by a maximal ramp incremental running test for determination, and 2) several (4-5) constant velocity running tests to determine VMLSS with a precision of 0.20 km·h-1. Determined BLRTs include LEmin and LEmin-related LEmin plus 1 (LEmin+1mM) and 1.5 mmol·L-1 (LEmin+1.5mM), along with well-established BLRTs such as conventionally-calculated LT, Dmax and fixed blood lactate concentration thresholds. LEmin did not differ from LT (P = 0.71; ES: 0.08) and was 27% lower than MLSS (P < 0.001; ES: 3.54). LEmin+1mM was not different from MLSS (P = 0.47; ES: 0.09). LEmin was the best predictor of VMLSS (r = 0.91; P < 0.001; SEE = 0.47 km·h-1), followed by LEmin+1mM (r = 0.86; P < 0.001; SEE = 0.58 km·h-1) and LEmin+1.5mM (r = 0.84; P < 0.001; SEE = 0.86 km·h-1). There was no statistical difference between MLSS and estimated MLSS using LEmin prediction formula (P = 0.99; ES: 0.001). Mean bias and limits of agreement were 0.00 ± 0.45 km·h-1 and ±0.89 km·h-1. Additionally, LEmin, LEmin+1mM and LEmin+1.5mM were the best predictors of (r = 0.72-0.79; P < 0.001). These results support LEmin, an objective submaximal overlooked and underused BLRT, to be one of the best single MLSS predictors in endurance trained runners. Our study advocates factors controlling LEmin to be shared, at least partly, with those controlling MLSS.
Keywords: Owles' point; aerobic capacity; aerobic threshold; anaerobic threshold; endurance assessment; lactate threshold; oxygen endurance performance limit; submaximal exercise testing.
Figures
References
-
- Barr D. P., Himwich H. E. (1923). Studies in the physiology of muscular exercise: III. Development and duration of changes in acid-base equilibrium. J. Biol. Chem. 55, 539–555
-
- Berg A., Jakob E., Lehmann M., Dickhuth H. H., Huber G., Keul J. (1990). Current aspects of modern ergometry. Pneumologie 44, 2–13. - PubMed
-
- Berg A., Stippig J., Keul J., Huber G. (1980). Zur Beurteilung der Leistungsfähigkeit und Belastbarkeit von Patienten mit coronarer Herzkrankheit. Dtsch. Z. Sportmed. 31, 199–205.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous