

Effectiveness and Safety of Compound Chinese Medicine plus Routine Western Medicine in In-Stent Restenosis: A Meta-Analysis and Systematic Review
- PMID: 30108660
- PMCID: PMC6077541
- DOI: 10.1155/2018/6207524
Effectiveness and Safety of Compound Chinese Medicine plus Routine Western Medicine in In-Stent Restenosis: A Meta-Analysis and Systematic Review
Abstract
Objective: To examine the effects and safety of oral compound Chinese medicine (CCM) plus routine western medicine (RWM) in in-stent restenosis (ISR).
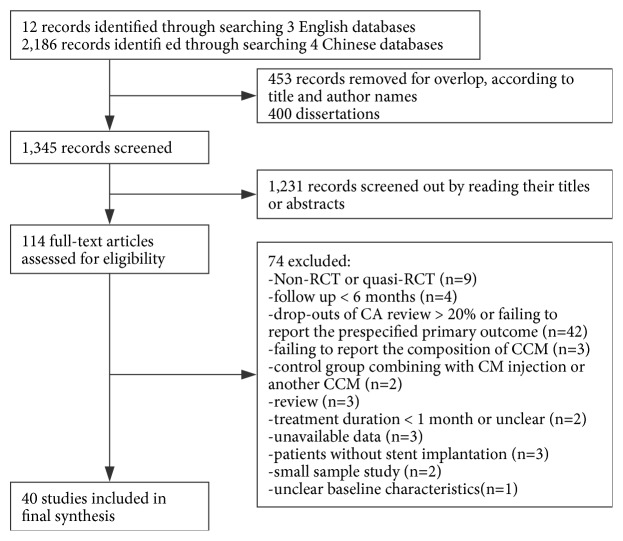
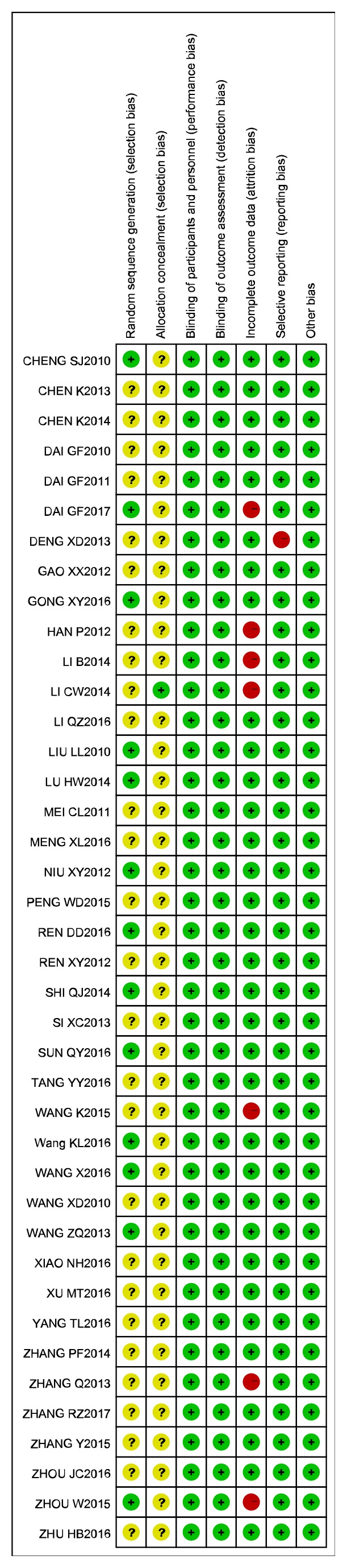
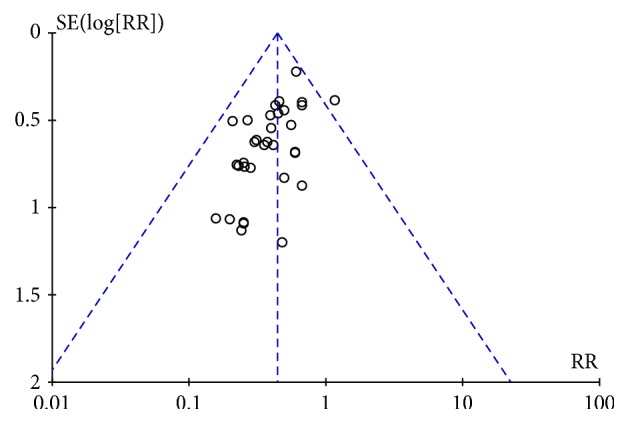
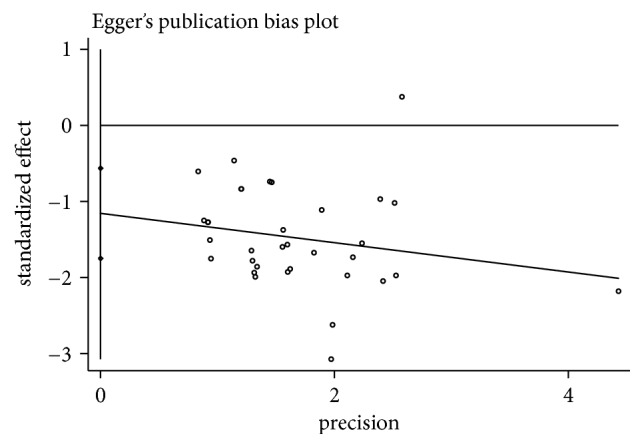
Methods: Various electronic databases (CBM, CNKI, VIP, Wanfang, PubMed, EMBASE, and Cochrane Library) were searched until April 2017. The quality of the included studies was evaluated, and meta-analyses were performed using RevMan5.3 and STATA 12.0 software. Moreover, funnel plot and Egger's publication bias plots were analysed to identify publication bias and adverse reactions were reported. A sensitive analysis was carried out according to the quality score.
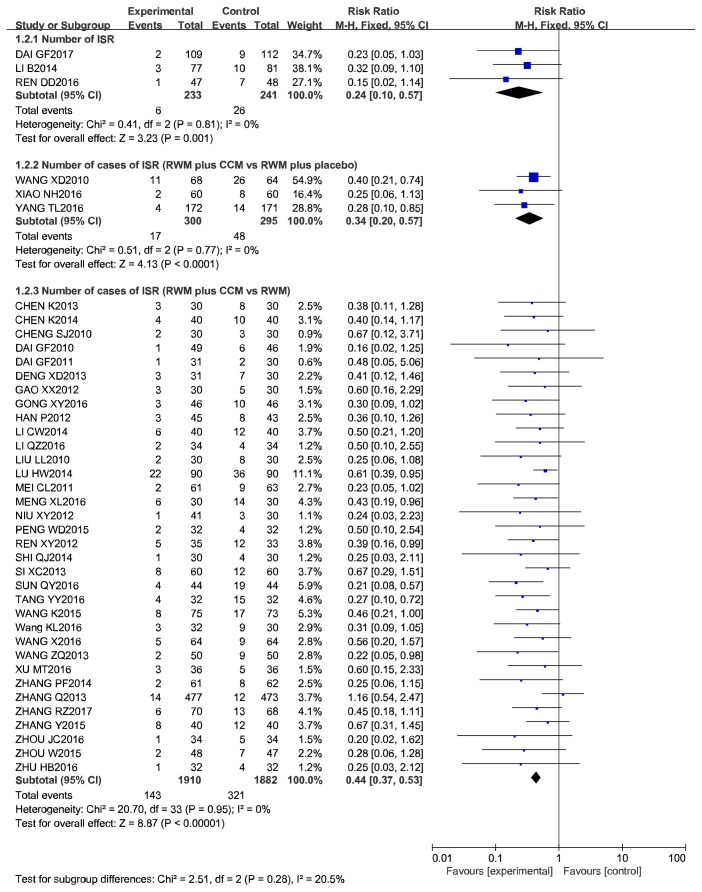
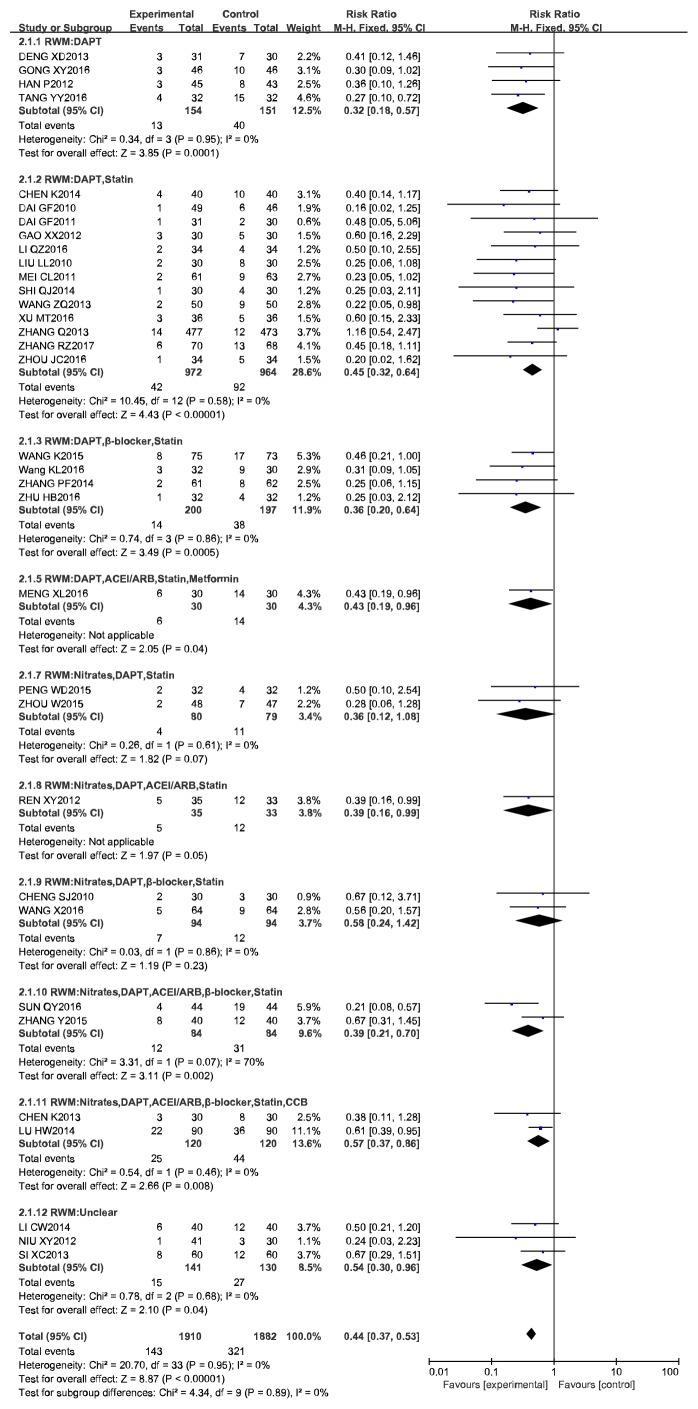
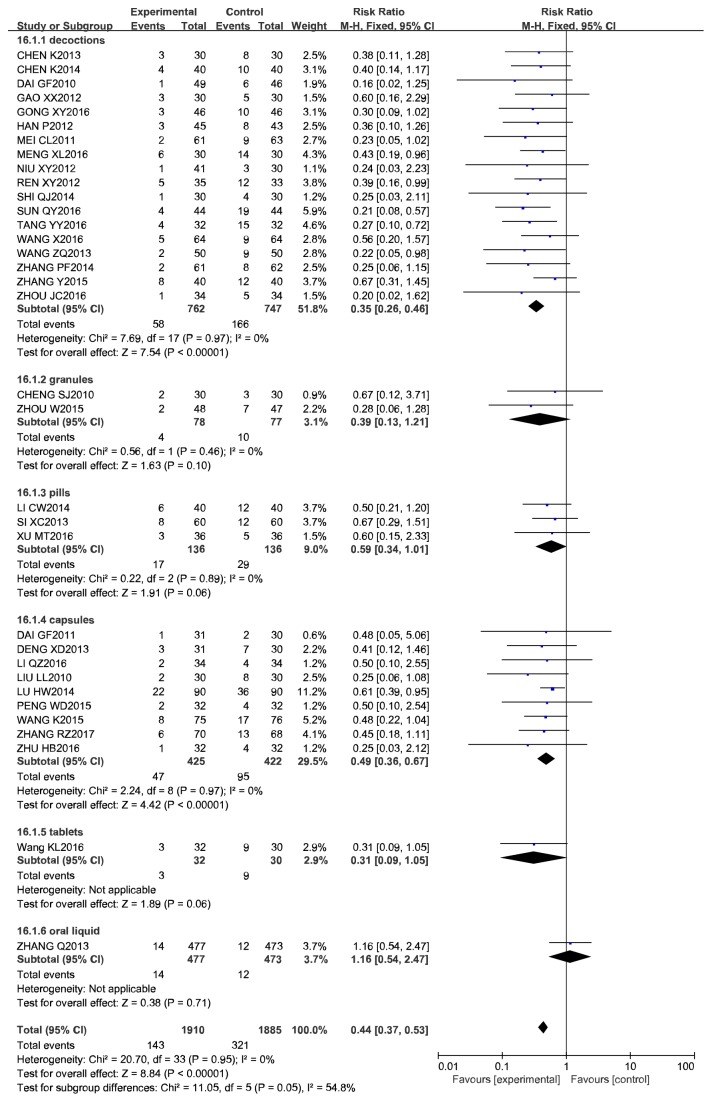
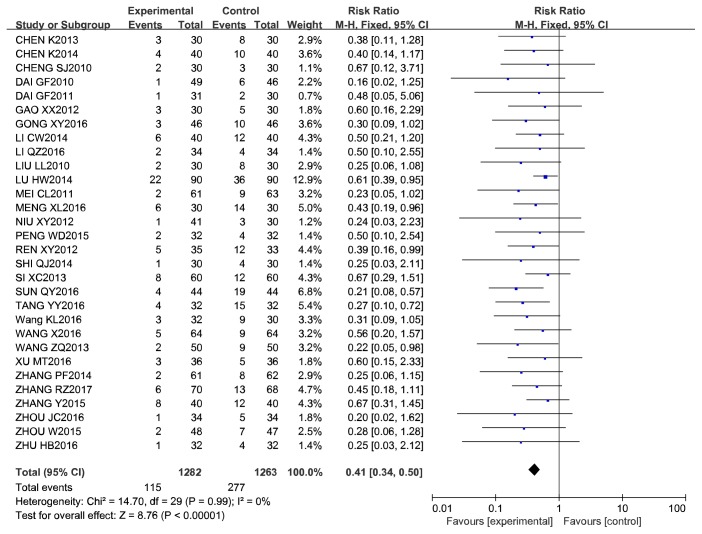
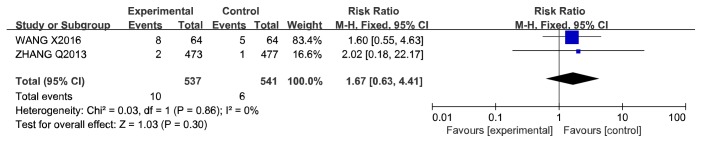
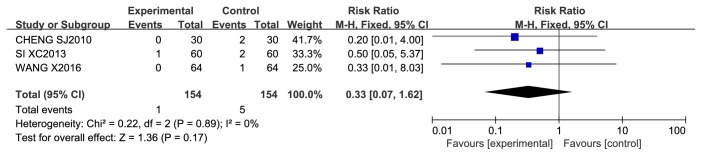
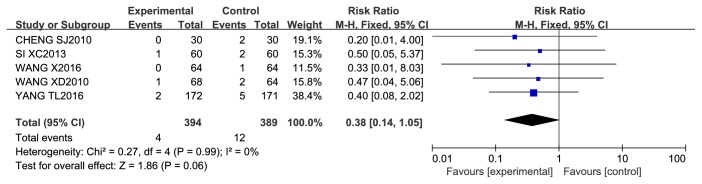
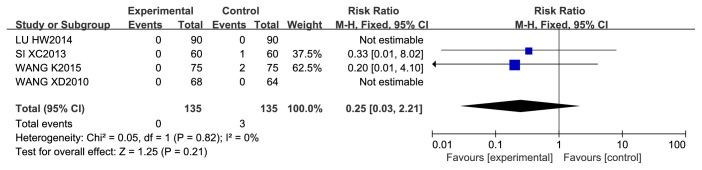
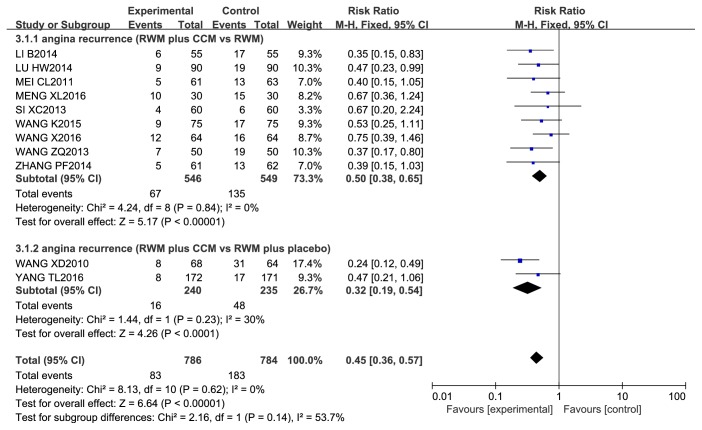
Results: In all, 40 RCTs involving 4536 patients were selected for this review. The pooled estimates of three studies showed that the benefit to the number of ISRs (NoR) was more substantial for CCM plus RWM than for RWM alone (RR 0.24, 95% CI 0.10 to 0.57, P = 0.001; I2 = 0%, P = 0.81). The rate of ISR was significantly lower for CCM plus RWM than for the same RWM alone (RR 0.44, 95% CI 0.37 to 0.53, P < 0.00001; I2 = 0%, P = 0.95). CCM plus RWM benefitted the rate of ISR when a CM placebo plus RWM was used as the control intervention (RR 0.34, 95% CI 0.20 to 0.57, P < 0.0001; I2 = 0%, P = 0.95). The difference of adverse reactions was not significant. For secondary outcomes, the CCM plus RWM group did not reduce the rates of revascularization and cardiac death, but it did reduce the rate of recurrent angina over the results observed in the RWM alone group. In addition, funnel plot and Egger's publication bias plot indicated that there was publication bias. The association between the use of CCM plus RWM and RWM alone remained significant after the sensitivity analysis excluding studies with low quality score (quality score ⩽ 4) with a pooled RR of 0.41 (95% CI, 0.34-0.50).
Conclusion: Oral CCM plus RWM clearly benefitted patients with percutaneous coronary intervention (PCI) because it prevented and treated ISR better than was observed for either RWM alone or a CM placebo plus RWM.
Figures
Similar articles
-
Tongxinluo capsule as supplementation and cardiovascular endpoint events in patients with coronary heart disease: A systematic review and meta-analysis of randomized, double-blind, placebo-controlled trials.J Ethnopharmacol. 2022 May 10;289:115033. doi: 10.1016/j.jep.2022.115033. Epub 2022 Jan 26. J Ethnopharmacol. 2022. PMID: 35091010
-
Pre-Percutaneous Coronary Intervention C-Reactive Protein Levels and In-Stent Restenosis: A Systematic Review and Meta-Analysis.Health Sci Rep. 2025 Apr 29;8(5):e70757. doi: 10.1002/hsr2.70757. eCollection 2025 May. Health Sci Rep. 2025. PMID: 40309624 Free PMC article. Review.
-
Efficacy and safety of yinqiao powder combined with western medicine in the treatment of pneumonia: A systematic review and meta-analysis.Complement Ther Clin Pract. 2021 Feb;42:101297. doi: 10.1016/j.ctcp.2020.101297. Epub 2020 Dec 16. Complement Ther Clin Pract. 2021. PMID: 33360842 Free PMC article.
-
Meta-analysis of therapeutic efficacy and effects of integrated traditional Chinese and Western medicine on coagulation and fibrinolysis system in patients with threatened abortion and polycystic ovary syndrome.Am J Transl Res. 2022 May 15;14(5):2768-2778. eCollection 2022. Am J Transl Res. 2022. PMID: 35702093 Free PMC article. Review.
-
Systematic Review of Chinese Herbal Medicines for Preventing in-Stent Coronary Restenosis after Percutaneous Coronary Intervention.Evid Based Complement Alternat Med. 2012;2012:253409. doi: 10.1155/2012/253409. Epub 2012 Feb 16. Evid Based Complement Alternat Med. 2012. PMID: 22454659 Free PMC article.
Cited by
-
Mechanistic exploration of Yiqi Liangxue Shengji prescription on restenosis after balloon injury by integrating metabolomics with network pharmacology.Pharm Biol. 2023 Dec;61(1):1260-1273. doi: 10.1080/13880209.2023.2244533. Pharm Biol. 2023. PMID: 37602438 Free PMC article.
References
-
- Wang X. Expert consensus on TCM diagnosis and treatment of chest pain after percutaneous coronary intervention (PCI) Journal of Traditional Chinese Medicine. 2014;55(13):1167–1170.
-
- Ren Y., Chen K.-J., Ruan X.-M. Systematic review of randomized controlled trials on preventing and treating restenosis after percutaneous coronary intervention with Chinese medicine. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi. 2008;28(7):597–601. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
