

Infected charcot spine arthropathy
- PMID: 30109137
- PMCID: PMC6082833
- DOI: 10.1038/s41394-018-0111-6
Infected charcot spine arthropathy
Abstract
Background: Charcot spinal arthropathy (CSA), a destructive spinal pathology, is seen in patients with impaired sensation. Superimposed infection in the affected spinal segments can lead to a challenge in the diagnosis and management. Spinal cord injury (SCI) is the leading cause of CSA as persons with SCI have significantly impaired sensation. Though infection of the CSA is rare, SCI persons are prone to superimposed infection of the Charcot spine. We report atypical presentations of three cases of CSA with superimposed infection.
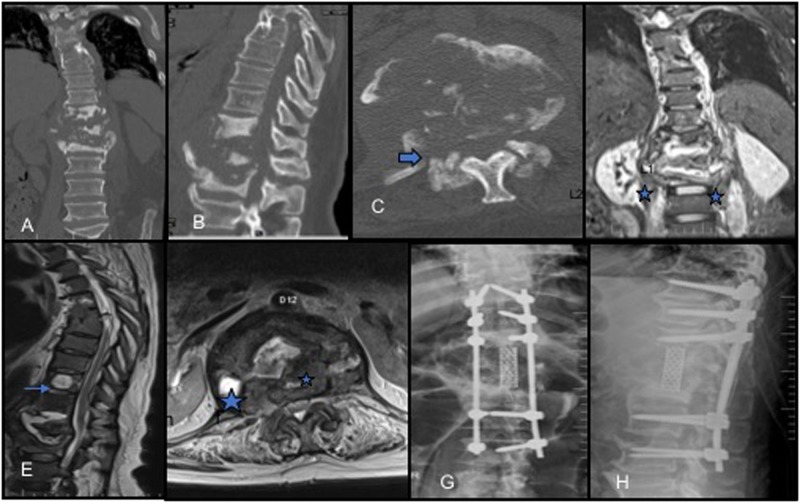
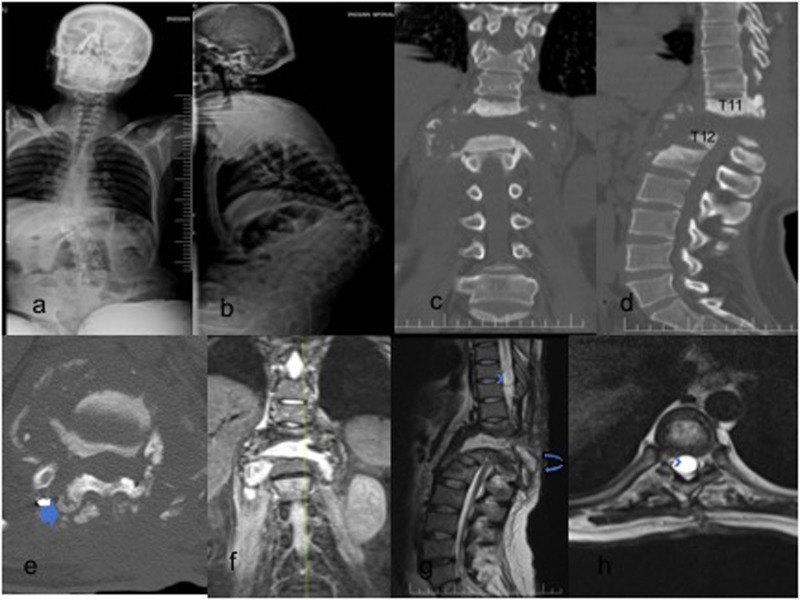
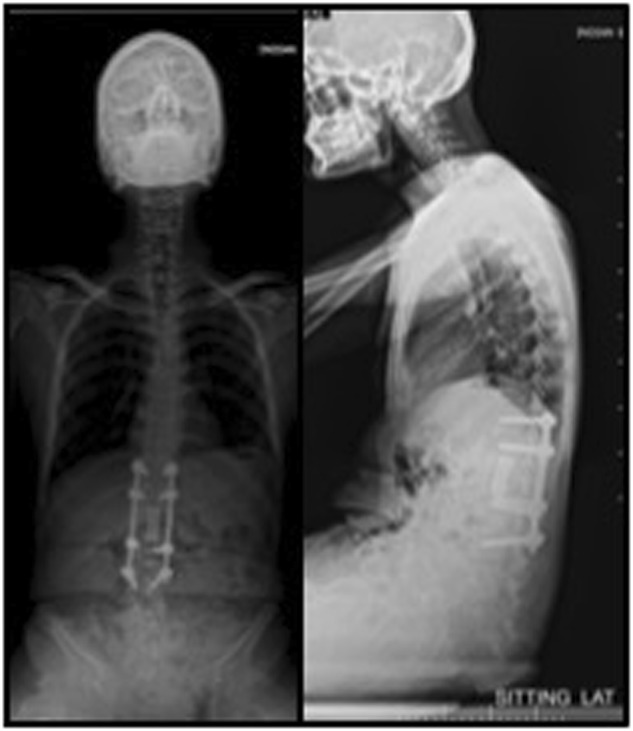
Case descriptions: A 47-year-old male with complete T7-8 SCI developed symptoms suggestive of infection and CSA. He was managed with a posterior vertebral column resection (PVCR) of T12 and intravenous antibiotics as the intraoperative culture showed the growth of E. coli and Pseudomonas. A 26-year-old male with T12 complete paraplegia, post status post open reduction and internal fixation with subsequent implants removal developed infection and CSA over the pseudo-arthrotic lesion with destruction of T12 and L1 vertebrae and an external fistulous track. He was managed with debridement and anterior column T11-L1 reconstruction with a Titanium cage and four-rod pedicle screw stabilization construct. A 25-year-old male with complete paraplegia with CSA at L4-S1. He underwent PVCR of L5 and L3-S2 posterior stabilization. The intraoperative culture and histopathology were suggestive of tuberculous infection.
Conclusion: Pyogenic or tubercular infection of CSA should be considered as a diagnostic possibility in persons with SCI who are more prone to infections. The management includes aggressive debridement and circumferential fusion along with appropriate medications to control the infection.
Conflict of interest statement
Compliance with ethical standardsThe authors declare that they have no conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
