

Bone Bruises in Children and Adolescents Not Associated With Ligament Ruptures [corrected]
- PMID: 30109238
- PMCID: PMC6083756
- DOI: 10.1177/2325967118786960
Bone Bruises in Children and Adolescents Not Associated With Ligament Ruptures [corrected]
Erratum in
-
Erratum.Orthop J Sports Med. 2019 Jan 31;7(1):2325967119831698. doi: 10.1177/2325967119831698. eCollection 2019 Jan. Orthop J Sports Med. 2019. PMID: 30783605 Free PMC article.
Abstract
Background: Clinical characteristics of uncomplicated bone bruises (ie, not associated with a ligament rupture, meniscal tear, or fracture of the knee) in young athletes have scarcely been reported.
Purpose: To identify mechanisms of injury, characterize bone bruise patterns, and identify clinical factors relating to recovery in young patients suffering uncomplicated bone bruises about the knee.
Study design: Case series; Level of evidence, 4.
Methods: A review of clinical records and magnetic resonance imaging (MRI) findings of patients seen at a single institution was completed.
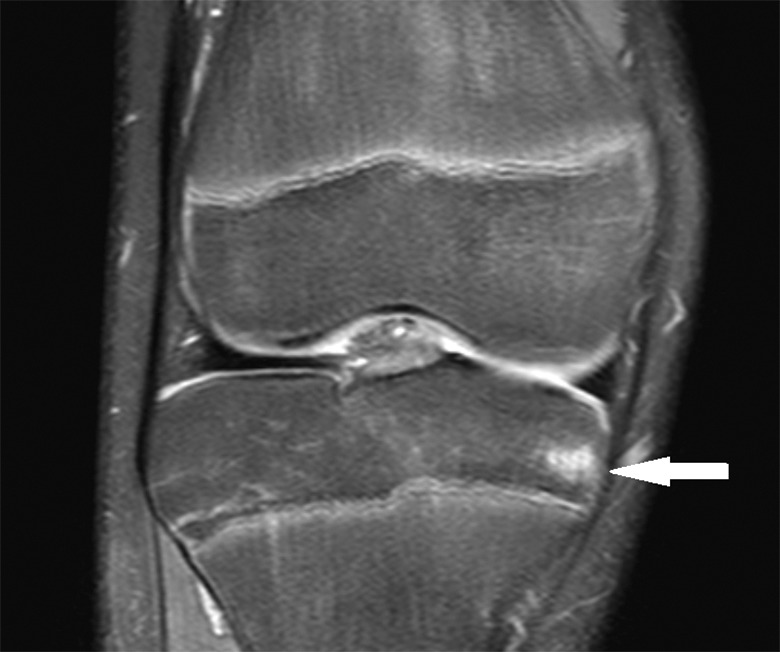
Results: We identified 62 children and teenagers (mean age, 13.9 years; range, 8-18 years) who had a total of 101 bone bruises on MRI. The injuries occurred during a variety of organized and recreational sporting activities, the most common being football, basketball, and soccer. The majority (61.4%) of bone bruises occurred as a result of noncontact mechanisms. Patients reported a mean pain scale score of 6.3 of 10 (range, 2-10) on presentation. Frequent clinical findings included non-joint-line tenderness (64.5%), limited range of motion (58.1%), joint-line tenderness (54.8%), and positive meniscal signs (50.0%). The majority of bone bruises (61.4%) were located medially, and the most common bone bruise type was subcortical (58.4%), followed by medullary/reticular (35.6%) and articular impaction (5.9%). The only factor related to time to recovery was mechanism of injury; patients reporting a noncontact mechanism required significantly more time to recover than those reporting a contact mechanism (mean, 99.7 ± 74.8 vs 65.7 ± 38.8 days, respectively; F = 3.753, P = .049).
Conclusion: In this case series of 62 pediatric patients with non-anterior cruciate ligament (ACL) bone bruises, the majority occurred in the medial compartment, suggesting that these bone bruises result from a mechanism distinct from the pivot-shift mechanism, classically thought to cause ACL injuries.
Keywords: MRI; adolescent; bone bruise; child; knee; pediatric sports medicine.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Figures



Similar articles
-
Association of Compartmental Bone Bruise Distribution With Concomitant Intra-articular and Extra-articular Injuries in Acute Anterior Cruciate Ligament Tears After Noncontact Sports Trauma.Orthop J Sports Med. 2018 Apr 24;6(4):2325967118767625. doi: 10.1177/2325967118767625. eCollection 2018 Apr. Orthop J Sports Med. 2018. PMID: 29780838 Free PMC article.
-
Posteromedial Tibial Bone Bruise After Anterior Cruciate Ligament Injury: An MRI Study of Bone Bruise Patterns in 208 Patients.Orthop J Sports Med. 2022 Oct 17;10(10):23259671221120636. doi: 10.1177/23259671221120636. eCollection 2022 Oct. Orthop J Sports Med. 2022. PMID: 36276425 Free PMC article.
-
Comparison Between Soccer and Basketball of Bone Bruise and Meniscal Injury Patterns in Anterior Cruciate Ligament Injuries.Orthop J Sports Med. 2021 Apr 14;9(4):2325967121995844. doi: 10.1177/2325967121995844. eCollection 2021 Apr. Orthop J Sports Med. 2021. PMID: 33912617 Free PMC article.
-
Clinical Implications of Bone Bruise Patterns Accompanying Anterior Cruciate Ligament Tears.Sports Health. 2022 Jul-Aug;14(4):585-591. doi: 10.1177/19417381211029583. Epub 2021 Jul 7. Sports Health. 2022. PMID: 34231443 Free PMC article. Review.
-
Bone Bruises Associated with Anterior Cruciate Ligament Injury as Indicators of Injury Mechanism: A Systematic Review.Sports Med. 2019 Mar;49(3):453-462. doi: 10.1007/s40279-019-01060-6. Sports Med. 2019. PMID: 30689129
References
-
- Ariyoshi M, Nagata K, Sato K, et al. Hemarthrosis of the knee and bone contusion. Kurume Med J. 1997;44:135–139. - PubMed
-
- Atkinson PJ, Cooper TG, Anseth S, Walter NE, Kargus R, Haut RC. Association of knee bone bruise frequency with time post-injury and type of soft tissue injury. Orthopedics. 2008;31(5):440. - PubMed
-
- Boks SS, Vroegindeweij D, Koes BW, Bernsen RMD, Hunink M, Bierma-Zeinstra SMA. Clinical consequences of posttraumatic bone bruise in the knee. Am J Sports Med. 2007;35(6):990–995. - PubMed
-
- Bretlau T, Tuxoe J, Larsen L, Jorgenson U, Thomsen HS, Lausten GS. Bone bruise in the acutely injured knee. Knee Surg Sports Traumatol Arthrosc. 2002;10:96–101. - PubMed
-
- Costa-Paz M, Muscolo L, Ayerza M, Makino A, Aponte-Tinao L. Magnetic resonance imaging follow-up study of bone bruises associated with anterior cruciate ligament ruptures. Arthroscopy. 2001;17(5):445–449. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
