

Platinum-based concurrent chemotherapy remains the optimal regimen for nasopharyngeal carcinoma: a large institutional-based cohort study from an endemic area
- PMID: 30109501
- PMCID: PMC11813322
- DOI: 10.1007/s00432-018-2721-6
Platinum-based concurrent chemotherapy remains the optimal regimen for nasopharyngeal carcinoma: a large institutional-based cohort study from an endemic area
Abstract
Purpose: To retrospectively investigate the optimal regimen of concurrent chemotherapy for nasopharyngeal carcinoma (NPC) by comparing clinical outcomes of patients who received platinum-based and non-platinum-based concurrent chemoradiotherapy (CCRT) regimens.
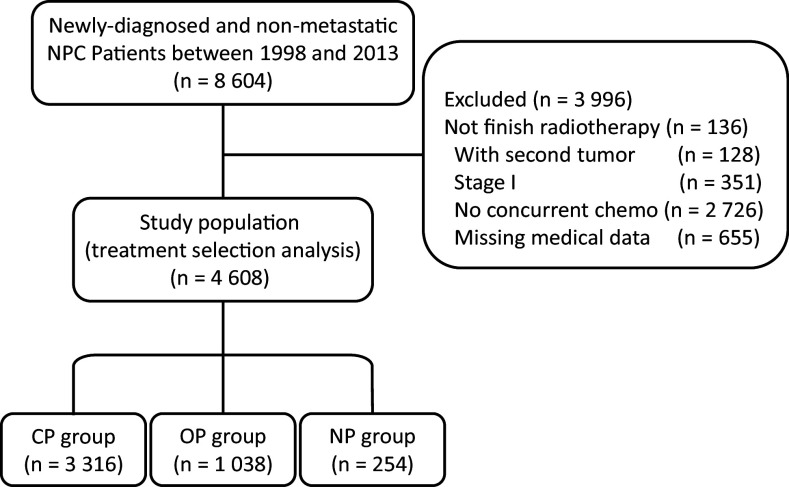
Methods: Based on a prospectively maintained database from 1998 to 2013 in an endemic area, a total of 4608 newly diagnosed, biopsy-proven, and non-disseminated NPC patients were identified and allocated into three cohorts based on concurrent chemotherapy regimens: cisplatin-based (CP) chemotherapy cohort, other platinum-based (OP) chemotherapy cohort, and non-platinum-based (NP) chemotherapy cohort. Overall survival (OS) and disease-free survival (DFS) were estimated using the Cox proportional hazards model and propensity score analysis of treatment using an inverse probability weighting model (PSA/IPTW). Finally, sensitivity analysis estimated the effects of potential unmeasured confounders.
Results: The median follow-up time was 68.5 months (range 2-194 months). The multivariate Cox model showed that NP regimens were significantly related with worse survival compared with CP or OP regimens (OS: HR 1.51, 95% CI 1.16-2.00, P = 0.002; HR 1.68, 95% CI 1.24-2.27, P = 0.001; DFS: HR 1.31, 95% CI 1.03-1.66, P = 0.031; HR 1.50, 95% CI 1.14-1.97, P = 0.004, respectively). Meanwhile, no significant survival difference was found between OP and CP regimens. The PSA/IPTW method, CCRT-specific and III-IVB NPC cohort subgroup analysis showed similar results. Sensitivity analysis confirmed the robustness of our results.
Conclusions: Platinum-based concurrent chemotherapy, including both CP and OP regimens, yields better survival benefits for non-metastatic NPC patients than the NP regimen and remains the optimal regimen for these patients.
Keywords: Cisplatin-based regimen; Concurrent chemoradiotherapy; Nasopharyngeal carcinoma; Propensity score analysis; Sensitivity analysis; Survival analysis.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



Similar articles
-
Induction chemotherapy plus IMRT alone versus induction chemotherapy plus IMRT-based concurrent chemoradiotherapy in locoregionally advanced nasopharyngeal carcinoma: a retrospective cohort study.J Cancer Res Clin Oncol. 2019 Jul;145(7):1857-1864. doi: 10.1007/s00432-019-02925-z. Epub 2019 May 6. J Cancer Res Clin Oncol. 2019. PMID: 31062162 Free PMC article.
-
Gemcitabine and cisplatin versus docetaxel and cisplatin as induction chemotherapy followed by concurrent chemoradiotherapy in locoregionally advanced nasopharyngeal carcinoma from non-endemic area of China.J Cancer Res Clin Oncol. 2020 Sep;146(9):2369-2378. doi: 10.1007/s00432-020-03229-3. Epub 2020 May 3. J Cancer Res Clin Oncol. 2020. PMID: 32363479 Free PMC article.
-
Chemotherapy for advanced gastric cancer.Cochrane Database Syst Rev. 2017 Aug 29;8(8):CD004064. doi: 10.1002/14651858.CD004064.pub4. Cochrane Database Syst Rev. 2017. PMID: 28850174 Free PMC article.
-
Platinum-containing regimens for metastatic breast cancer.Cochrane Database Syst Rev. 2017 Jun 23;6(6):CD003374. doi: 10.1002/14651858.CD003374.pub4. Cochrane Database Syst Rev. 2017. PMID: 28643430 Free PMC article.
-
Comparison of TPF and PF induction chemotherapy combined with cisplatin concurrent chemoradiotherapy for locoregionally advanced nasopharyngeal carcinoma: A systematic review and meta-analysis.Medicine (Baltimore). 2025 Jan 17;104(3):e41278. doi: 10.1097/MD.0000000000041278. Medicine (Baltimore). 2025. PMID: 39833074 Free PMC article.
Cited by
-
Raltitrexed versus 5-fluorouracil with cisplatin and concurrent radiotherapy for locally advanced nasopharyngeal carcinoma: An open labeled, randomized, controlled, and multicenter clinical trial.Cancer Med. 2020 Sep;9(17):6166-6172. doi: 10.1002/cam4.3260. Epub 2020 Jul 12. Cancer Med. 2020. PMID: 32657029 Free PMC article. Clinical Trial.
-
Role of concurrent chemoradiation on locally advanced unresectable adenoid cystic carcinoma.Korean J Intern Med. 2021 Jan;36(1):175-181. doi: 10.3904/kjim.2019.104. Epub 2020 Mar 30. Korean J Intern Med. 2021. PMID: 32218101 Free PMC article.
-
DW-MRI-Guided Dose Escalation Improves Local Control of Locally Advanced Nasopharyngeal Carcinoma Treated with Chemoradiotherapy.Cancer Manag Res. 2020 May 6;12:3107-3116. doi: 10.2147/CMAR.S239033. eCollection 2020. Cancer Manag Res. 2020. PMID: 32440209 Free PMC article.
-
MiRNAs in Radiotherapy Resistance of Nasopharyngeal Carcinoma.J Cancer. 2020 Apr 6;11(13):3976-3985. doi: 10.7150/jca.42734. eCollection 2020. J Cancer. 2020. PMID: 32328201 Free PMC article. Review.
References
-
- Adelstein D et al (2017) NCCN guidelines insights: head and neck cancers, version 2.2017. J Natl Compr Cancer Netw 15:761–770. 10.6004/jnccn.2017.0101 - PubMed
-
- Al-Sarraf M et al (1998) Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized intergroup study 0099. J Clin Oncol 16:1310–1317 - PubMed
-
- Blanchard P et al (2015) Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the MAC-NPC meta-analysis. Lancet Oncol 16:645–655. 10.1016/S1470-2045(15)70126-9 - PubMed
MeSH terms
Substances
Grants and funding
- 81572665/National Natural Science Foundation of China
- 81172041/National Natural Science Foundation of China
- 81472525/National Natural Science Foundation of China
- 2014A050503033/International Cooperation Project of Science and Technology Plan of Guangdong Province
- 2016A050502011/International Cooperation Project of Science and Technology Plan of Guangdong Province
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
