

Aiming to Improve Readmissions Through InteGrated Hospital Transitions (AIRTIGHT): a Pragmatic Randomized Controlled Trial
- PMID: 30109585
- PMCID: PMC6318199
- DOI: 10.1007/s11606-018-4617-1
Aiming to Improve Readmissions Through InteGrated Hospital Transitions (AIRTIGHT): a Pragmatic Randomized Controlled Trial
Abstract
Background: Despite years of intense focus, inpatient and observation readmission rates remain high and largely unchanged. Hospitals have little, robust evidence to guide the selection of interventions effective at reducing 30-day readmissions in real-world settings.
Objective: To evaluate if implementation of recent recommendations for hospital transition programs is effective at reducing 30-day readmissions in a population discharged to home and at high-risk for readmission.
Design: A non-blinded, pragmatic randomized controlled trial ( Clinicaltrials.gov : NCT02763202) conducted at two hospitals in Charlotte, North Carolina.
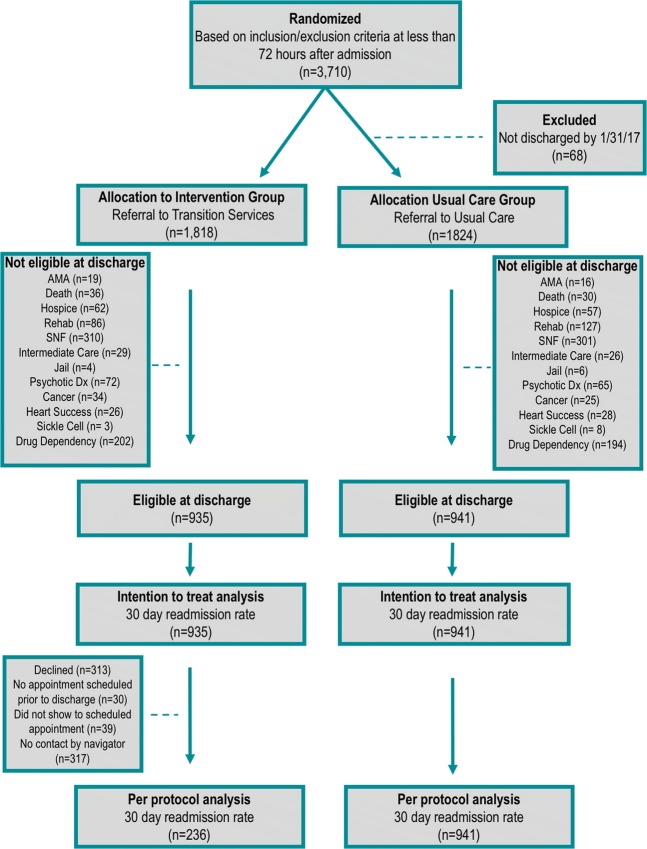
Patients: A total of 1876 adult patients, under the care of a hospitalist, and at high risk for readmissions.
Intervention: Random allocation to a Transition Services (TS) program (n = 935) that bridges inpatient, outpatient, and home settings, providing patients virtual and in-person access to a dedicated multidisciplinary team for 30-days, or usual care (n = 941).
Main measure: Thirty-day, unplanned, inpatient, or observation readmission rate.
Key results: The 30-day readmission rate was 15.2% in the TS group and 16.3% in the usual care group (RR 0.93; 95% [CI, 0.76 to 1.15]; P = 0.52). There were no significant differences in readmissions at 60 and 90 days or in 30-day Emergency Department visit rates. Patients, who were referred to TS and readmitted, had less Intensive Care Unit admissions 15.5% vs. 26.8% (RR 0.74; 95% [CI, 0.59 to 0.93]; P = 0.02).
Conclusions: An intervention inclusive of contemporary recommendations does not reduce a high-risk population's 30-day readmission rate. The high crossover to usual care (74.8%) reflects the challenge of non-participation that is ubiquitous in the real-world implementation of population health interventions.
Trial registry: ClinicalTrials.gov ; registration ID number: NCT02763202, URL: https://clinicaltrials.gov/ct2/show/NCT02763202.
Keywords: healthcare value; outcomes research; population health; pragmatic research; readmissions.
Conflict of interest statement
AM has received funding support for research from AstraZeneca, Amylin Pharmaceuticals, and is a cofounder of iEnroll, LLC. No other authors report any potential conflicts of interest.
Comment in
-
Finding Joy in the Practice of Implementation Science: What Can We Learn from a Negative Study?J Gen Intern Med. 2019 Jan;34(1):9-11. doi: 10.1007/s11606-018-4715-0. J Gen Intern Med. 2019. PMID: 30357591 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
