

Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: a patient-level meta-analysis of randomized trials
- PMID: 30111341
- PMCID: PMC6092799
- DOI: 10.1186/s13054-018-2125-7
Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: a patient-level meta-analysis of randomized trials
Abstract
Background: The clinical utility of serum procalcitonin levels in guiding antibiotic treatment decisions in patients with sepsis remains unclear. This patient-level meta-analysis based on 11 randomized trials investigates the impact of procalcitonin-guided antibiotic therapy on mortality in intensive care unit (ICU) patients with infection, both overall and stratified according to sepsis definition, severity, and type of infection.
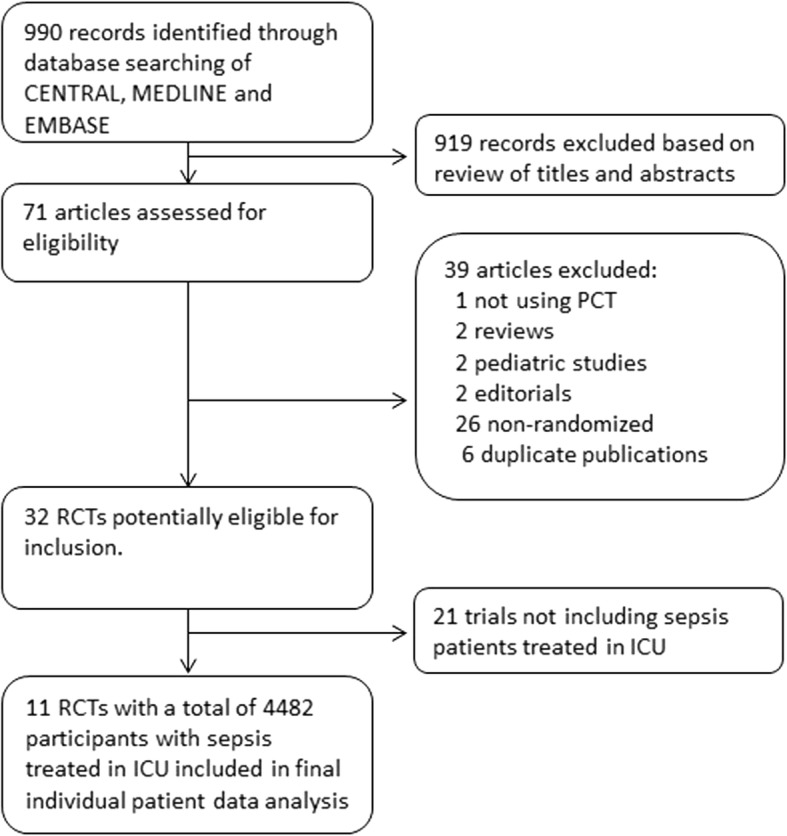
Methods: For this meta-analysis focusing on procalcitonin-guided antibiotic management in critically ill patients with sepsis of any type, in February 2018 we updated the database of a previous individual patient data meta-analysis which was limited to patients with respiratory infections only. We used individual patient data from 11 trials that randomly assigned patients to receive antibiotics based on procalcitonin levels (the "procalcitonin-guided" group) or the current standard of care (the "controls"). The primary endpoint was mortality within 30 days. Secondary endpoints were duration of antibiotic treatment and length of stay.
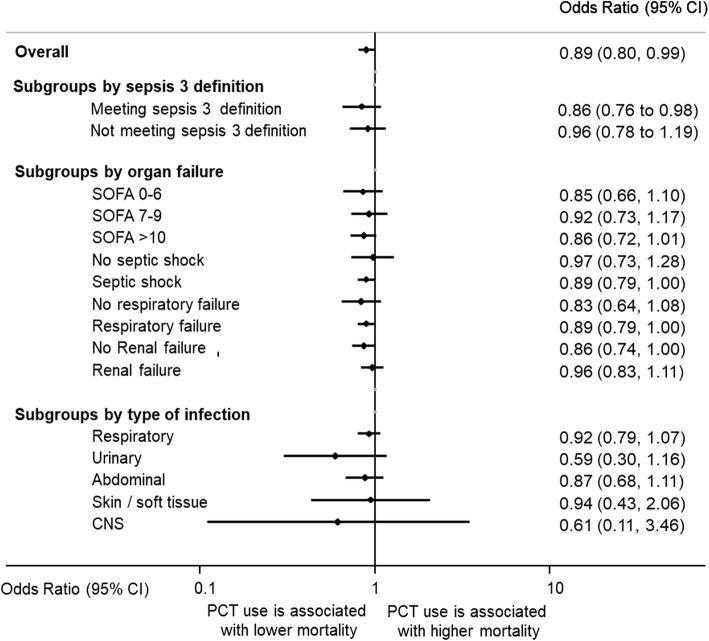
Results: Mortality in the 2252 procalcitonin-guided patients was significantly lower compared with the 2230 control group patients (21.1% vs 23.7%; adjusted odds ratio 0.89, 95% confidence interval (CI) 0.8 to 0.99; p = 0.03). These effects on mortality persisted in a subgroup of patients meeting the sepsis 3 definition and based on the severity of sepsis (assessed on the basis of the Sequential Organ Failure Assessment (SOFA) score, occurrence of septic shock or renal failure, and need for vasopressor or ventilatory support) and on the type of infection (respiratory, urinary tract, abdominal, skin, or central nervous system), with interaction for each analysis being > 0.05. Procalcitonin guidance also facilitated earlier discontinuation of antibiotics, with a reduction in treatment duration (9.3 vs 10.4 days; adjusted coefficient -1.19 days, 95% CI -1.73 to -0.66; p < 0.001).
Conclusion: Procalcitonin-guided antibiotic treatment in ICU patients with infection and sepsis patients results in improved survival and lower antibiotic treatment duration.
Keywords: Antibiotic stewardship; Meta-analysis; Procalcitonin; Sepsis.
Conflict of interest statement
Ethics approval and consent to participate
All trial included in the meta-analysis enrolled patients providing informed consent and had approval from their institutional review boards.
Consent for publication
Not applicable.
Competing interests
BioMérieux Inc. provided an unrestricted research grant to conduct this analysis. However, no personnel from the company were involved in the conduct of the analysis or in the preparation of the manuscript. PS and BM have received support from Thermo-Fisher and BioMérieux to attend meetings and fulfill speaking engagements. BM has also served as a consultant to BioMérieux and Thermo-Fisher. SS has received lecture fees and research support from Thermo-Fisher. CEL has received lecture fees from Brahms and Merck Sharp & Dohme-Chibret. JC has received consulting and lecture fees from Pfizer, Brahms, Wyeth, Johnson & Johnson, Nektar-Bayer, and Arpida. MW has received consulting and lectures fees from Merck Sharp & Dohme-Chibret, Janssen-Cilag, Gilead, Astellas, Sanofi, and Thermo-Fisher. YS has received unrestricted research grants from Thermo-fisher, BioMérieux, Orion Pharma, and Pfizer. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Shehabi Y, Sterba M, Garrett PM, Rachakonda KS, Stephens D, Harrigan P, Walker A, Bailey MJ, Johnson B, Millis D, et al. Procalcitonin algorithm in critically ill adults with undifferentiated infection or suspected sepsis. A randomized controlled trial. Am J Respir Crit Care Med. 2014;190(10):1102–1110. doi: 10.1164/rccm.201408-1483OC. - DOI - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Schuetz P, Birkhahn R, Sherwin R, Jones AE, Singer A, Kline JA, Runyon MS, Self WH, Courtney DM, Nowak RM, et al. Serial procalcitonin predicts mortality in severe sepsis patients: results from the multicenter procalcitonin MOnitoring SEpsis (MOSES) study. Crit Care Med. 2017;45(5):781–789. doi: 10.1097/CCM.0000000000002321. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
