

Eosinophilic Myocarditis Demonstrated Using Cardiac Magnetic Resonance Imaging in a Patient with Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss Disease)
- PMID: 30112268
- PMCID: PMC6089482
- DOI: 10.7759/cureus.2792
Eosinophilic Myocarditis Demonstrated Using Cardiac Magnetic Resonance Imaging in a Patient with Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss Disease)
Abstract
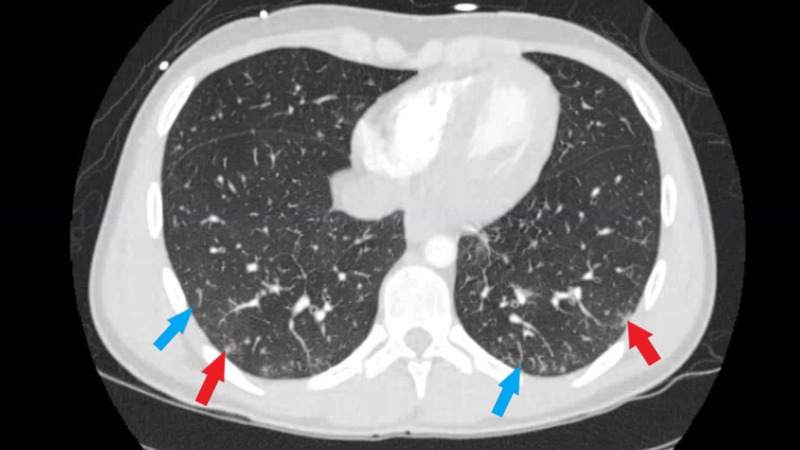
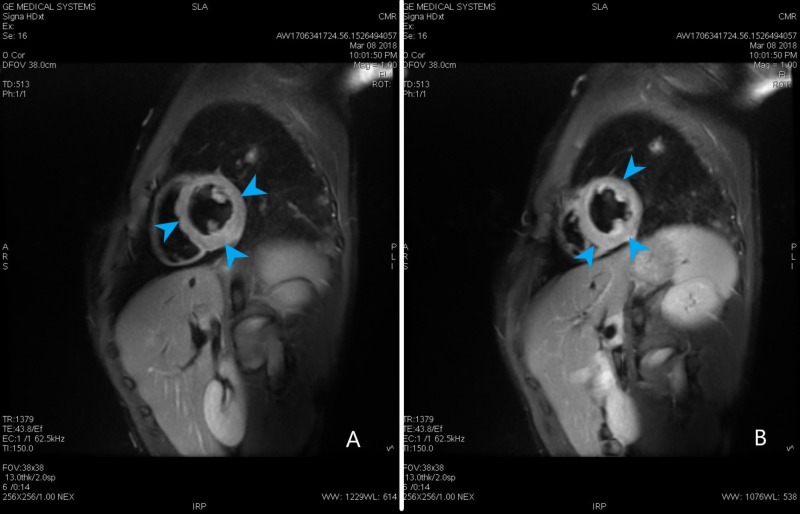
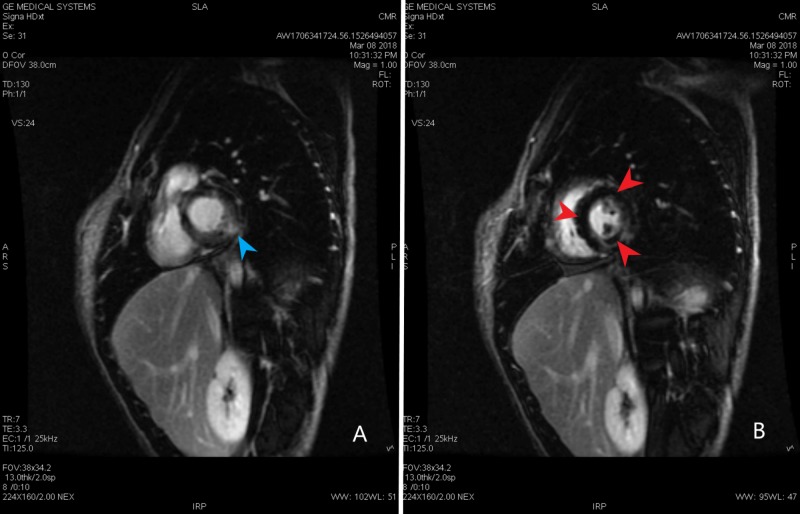
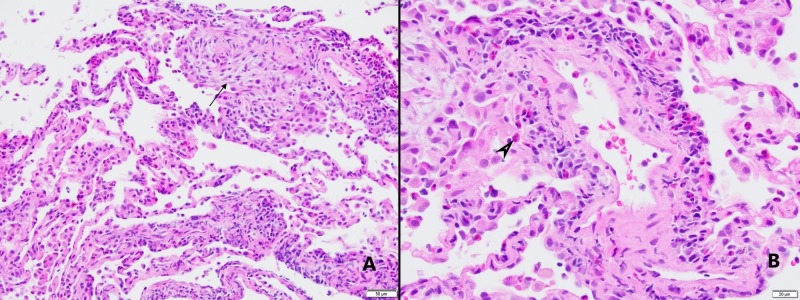
Eosinophilic granulomatosis with polyangiitis (EGPA), historically known as the Churg-Strauss disease, is a small- to medium-sized vessel multi-organ vasculitis with a propensity to involve the heart. EGPA is a rare condition with an estimated annual incidence of one to 4.2 people per million. The cardiac involvement causes significant morbidity and mortality in EGPA patients. Approximately 50% of the deaths in EGPA are related to cardiac disease and occur within the first few months since diagnosis. The current recommendations support evaluation of cardiac involvement by using history, physical exam and multimodality imaging including echocardiogram and cardiac magnetic resonance imaging (CMR). Here, we report a rare case of eosinophilic myocarditis in a 19-year-old patient with EGPA seen on CMR. Pertinent literature is also reviewed. We highlighted the importance of CMR in diagnosing and follow up of EGPA patients.
Keywords: cardiac magnetic resonance imaging; churg strauss disease; coronary cta; egpa; elevated troponins; eosinophilic myocarditis; five factor score.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
The Critical Role of Cardiac Magnetic Resonance Imaging in Evaluating Patients With Eosinophilic Granulomatosis With Polyangiitis.Cureus. 2020 Sep 6;12(9):e10279. doi: 10.7759/cureus.10279. Cureus. 2020. PMID: 33042714 Free PMC article. Review.
-
Comprehensive evaluation of cardiac involvement in eosinophilic granulomatosis with polyangiitis (EGPA) with cardiac magnetic resonance.Eur J Intern Med. 2017 Apr;39:51-56. doi: 10.1016/j.ejim.2016.09.014. Epub 2016 Oct 7. Eur J Intern Med. 2017. PMID: 27727077
-
Acute heart failure due to fulminant eosinophilic myocarditis with mononeuritis: eosinophilic granulomatosis with polyangiitis requiring cardiac multimodality imaging and systemic evaluation: a case report.Eur Heart J Case Rep. 2025 Jan 17;9(2):ytaf010. doi: 10.1093/ehjcr/ytaf010. eCollection 2025 Feb. Eur Heart J Case Rep. 2025. PMID: 39925776 Free PMC article.
-
Detecting cardiac involvement with magnetic resonance in patients with active eosinophilic granulomatosis with polyangiitis.Int J Cardiovasc Imaging. 2016 Jun;32 Suppl 1:155-62. doi: 10.1007/s10554-016-0843-y. Epub 2016 Feb 1. Int J Cardiovasc Imaging. 2016. PMID: 26831057
-
Diagnosis and classification of eosinophilic granulomatosis with polyangiitis (formerly named Churg-Strauss syndrome).J Autoimmun. 2014 Feb-Mar;48-49:99-103. doi: 10.1016/j.jaut.2014.01.018. Epub 2014 Feb 12. J Autoimmun. 2014. PMID: 24530234 Review.
Cited by
-
Initial Hemorrhagic Pericardial Effusion Evolving Into Perimyocarditis: An Atypical Early Presentation of Eosinophilic Granulomatosis With Polyangiitis.Cureus. 2025 Jul 17;17(7):e88155. doi: 10.7759/cureus.88155. eCollection 2025 Jul. Cureus. 2025. PMID: 40821336 Free PMC article.
-
The Critical Role of Cardiac Magnetic Resonance Imaging in Evaluating Patients With Eosinophilic Granulomatosis With Polyangiitis.Cureus. 2020 Sep 6;12(9):e10279. doi: 10.7759/cureus.10279. Cureus. 2020. PMID: 33042714 Free PMC article. Review.
-
The Diagnostic Challenge of Eosinophilic Granulomatosis With Polyangiitis Presenting as Acute Eosinophilic Myocarditis: Case Report and Literature Review.Front Cardiovasc Med. 2022 Jul 7;9:913724. doi: 10.3389/fcvm.2022.913724. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35872900 Free PMC article.
-
Management of Coronary Artery Diseases in Systemic Vasculitides: Complications and Strategies.Medicina (Kaunas). 2024 Sep 25;60(10):1574. doi: 10.3390/medicina60101574. Medicina (Kaunas). 2024. PMID: 39459361 Free PMC article. Review.
-
MR and CT angiography in the diagnosis of vasculitides.BJR Open. 2023 Sep 25;5(1):20220020. doi: 10.1259/bjro.20220020. eCollection 2023. BJR Open. 2023. PMID: 37953869 Free PMC article. Review.
References
-
- Allergic granulomatosis, allergic angiitis, and periarteritis nodosa. Churg J, Strauss L. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1937314/ Am J Pathol. 1951;27:277–301. - PMC - PubMed
-
- Churg-Strauss syndrome. Greco A, Rizzo MI, De Virgilio A, et al. Autoimmun Rev. 2015;14:341–348. - PubMed
-
- Diagnosis and classification of eosinophilic granulomatosis with polyangiitis (formerly named Churg-Strauss syndrome) Mouthon L, Dunogue B, Guillevin L. J Autoimmun. 2014;48:99–103. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources