

Lowering blood pressure in primary care in Vienna (LOW-BP-VIENNA) : A cluster-randomized trial
- PMID: 30112584
- PMCID: PMC6290730
- DOI: 10.1007/s00508-018-1374-4
Lowering blood pressure in primary care in Vienna (LOW-BP-VIENNA) : A cluster-randomized trial
Abstract
Background: In Austria only 41% of patients with treated hypertension (HTN) have their blood pressure (BP) controlled. This study investigated a strategy to improve BP control in primary care.
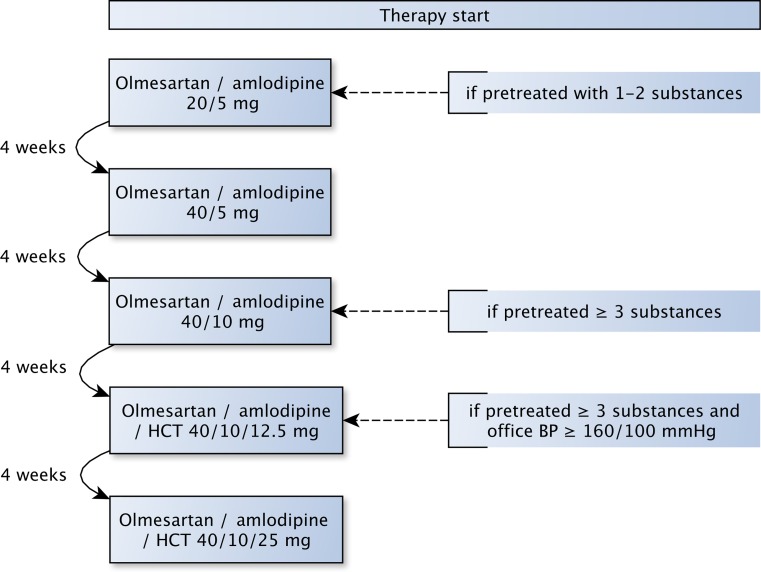
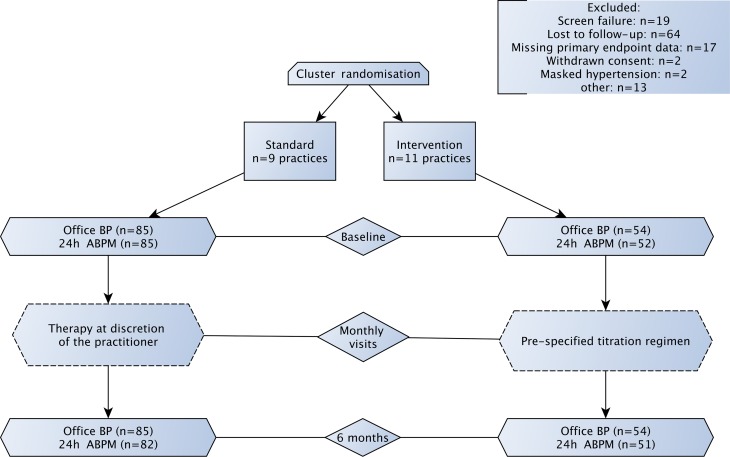
Methods: General practitioners (GPs) were randomized to interventional care vs. standard care and included patients with uncontrolled office BP > 140/90 mm Hg. In interventional care, antihypertensive therapy was up-titrated using a single pill combination (olmesartan, amlodipine and/or hydrochlorothiazde) in 4‑week intervals. In standard care, physicians were encouraged to treat according to the 2013 European Society of Cardiology guidelines for the management of arterial hypertension. The primary endpoint was the proportion of patients with controlled office BP < 140/90 mm Hg at 6 months. The main secondary endpoint was the improvement in 24 h ambulatory BP (ABPM, Clinicaltrials.gov NCT02377661).
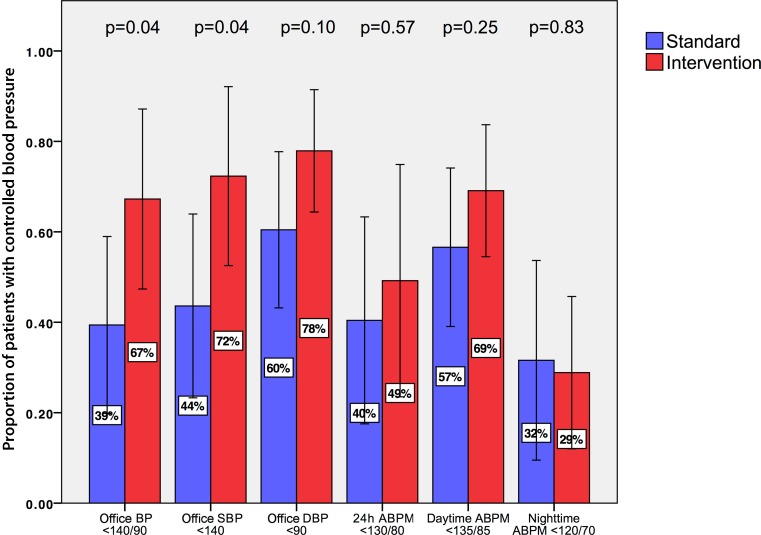
Results: Between 2015-2017, 20 GPs contributed to patient recruitment. The trial was discontinued due to slow recruitment after inclusion of 139 eligible patients, 54 of whom were included in the interventional group. A significantly larger proportion of patients in interventional vs. standard care achieved the office BP target (67% ± 26% vs. 39% ± 29%, respectively, mean difference -27.9%, 95% confidence interval CI -54.0%; -1.7%, p = 0.038). The proportion of patients with controlled 24 h ABPM (<130/80 mm Hg) was similar between groups (49% ± 33% vs. 40% ± 34%, respectively, mean difference -8.8%, 95% CI -40.7%; 23.1%, p = 0.57). At baseline, pretreated patients received an average of 1.5 ± 0.8 vs. 1.7 ± 0.9 antihypertensive prescriptions. At 6 months, the respective BP reductions were achieved with 1.2 ± 0.5 prescriptions in interventional vs. 2.0 ± 1.0 in standard care (p < 0.01).
Conclusion: In both groups statistically and clinically significant BP reductions were observed after 6 months. In the interventional care group, a larger proportion of patients achieved the office BP target compared to standard care. The 24 h ambulatory blood pressure levels were controlled in 44% of patients at 6 months, without significant differences between groups. The respective BP reductions were achieved with a significantly lower medication burden in interventional care.
Keywords: Ambulatory blood pressure measurement; Arterial hypertension; Disease management programs; Hypertension control; Single pill combination drugs.
Conflict of interest statement
M. Rohla received advisory fees from Daiichi Sankyo and Novartis, and lecturing fees from Biotronik and Takeda Pharma, all outside the submitted work. K. Huber received lecturing fees and advisory honoraria from Boehringer Ingelheim, Pfizer/BMS, Bayer, Daiichi Sankyo, Sanofi-Aventis, AstraZeneca, and Eli Lilly. T.W. Weiss received lecturing fees and advisory fees from Daiichi Sankyo, Boehringer Ingelheim and Pfizer/BMS. M. Tscharre declares that he has no competing interests.
Figures

References
-
- Banegas JR, Lopez-Garcia E, Dallongeville J, Guallar E, Halcox JP, Borghi C, et al. Achievement of treatment goals for primary prevention of cardiovascular disease in clinical practice across Europe: The EURIKA study. Eur Heart J. 2011;32(17):2143–2152. doi: 10.1093/eurheartj/ehr080. - DOI - PMC - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies C. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi: 10.1016/S0140-6736(02)11911-8. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
