

Laparoscopic inguinal hernia repair: a rare case of colonic mesh migration
- PMID: 30112945
- PMCID: PMC6204502
- DOI: 10.1308/rcsann.2018.0135
Laparoscopic inguinal hernia repair: a rare case of colonic mesh migration
Abstract
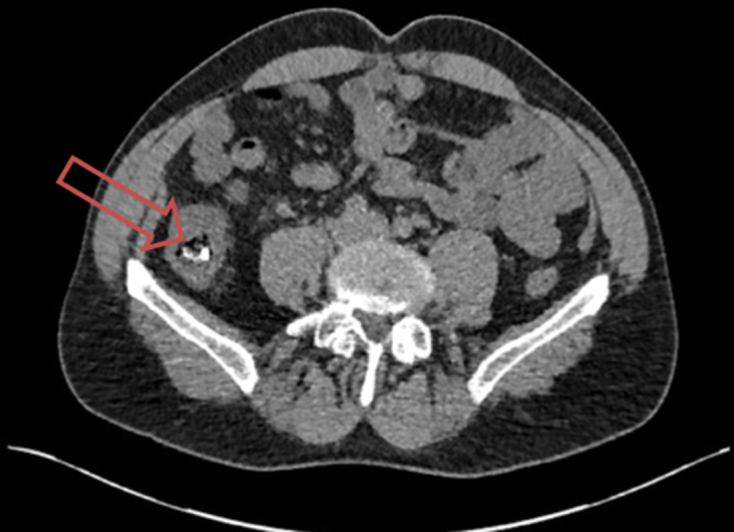
Inguinal hernia repair can be performed via either an open or laparoscopic technique. Use of a mesh to repair the abdominal wall defect is now common practice, leading to a reduction in hernia recurrence but also associated with a number of complications. We report a rare case of a 49-year old man who presented 3 years after laparoscopic hernia repair with right-sided abdominal pain and loose stools. Colonoscopy and computed tomography revealed a mesh and fixation devices within the lumen of the caecum and ascending colon. The mesh was successfully excised with primary closure of the bowel defect. This case highlights the importance of recognising mesh migration as a complication of hernia repair, a phenomenon which can lead to serious morbidity. We suggest that patients should be informed of this risk during the consent process, while further research is needed to investigate how this occurrence can be prevented.
Keywords: Inguinal hernia; Laparoscopic; Mesh migration; Totally extraperitoneal; Transabdominal preperitoneal.
Figures




References
-
- Kingsnorth A, LeBlanc K. Hernias: inguinal and incisional. Lancet 2003; (9395): 1,561–1,571. - PubMed
-
- Neumayer L, Giobbie-Hurder A, Jonasson O, Fitzgibbons R Jr, Dunlop D, Gibbs J et al. . Open mesh versus laparoscopic mesh repair of inguinal hernia. The New England journal of medicine 2004; (18): 1,819–1,827. - PubMed
-
- Agrawal A, Avill R. Mesh migration following repair of inguinal hernia: a case report and review of literature. Hernia 2005; (1): 79–82. - PubMed
-
- Peiper CH, Klinge U, Junge K, Schumpelick V. Meshes in inguinal hernia repair. Zentralblatt für Chirurgie 2002; (7): 573–577. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources