

Frailty Phenotypes and Relations With Surgical Outcomes: A Latent Class Analysis
- PMID: 30113393
- PMCID: PMC6931904
- DOI: 10.1213/ANE.0000000000003695
Frailty Phenotypes and Relations With Surgical Outcomes: A Latent Class Analysis
Abstract
Background: Frailty is an important concept in the care of older adults although controversy remains regarding its defining features and clinical utility. Both the Fried phenotype and the Rockwood deficit accumulation approaches cast frailty as a "burden" without exploring the relative salience of its cardinal markers and their relevance to the patient. New multifactorial perspectives require a reliable assessment of frailty that can validly predict postoperative health outcomes.
Methods: In a retrospective study of 2828 unselected surgical patients, we used item response theory to examine the ability of 32 heterogeneous markers capturing limitations in physical, functional, emotional, and social activity domains to indicate severity of frailty as a latent continuum. Eighteen markers efficiently indicated frailty severity and were then subject to latent class analysis to derive discrete phenotypes. Next, we validated the obtained frailty phenotypes against patient-reported 30-day postoperative outcomes using multivariable logistic regression. Models were adjusted for demographics, comorbidity, type and duration of surgery, and cigarette and alcohol consumption.
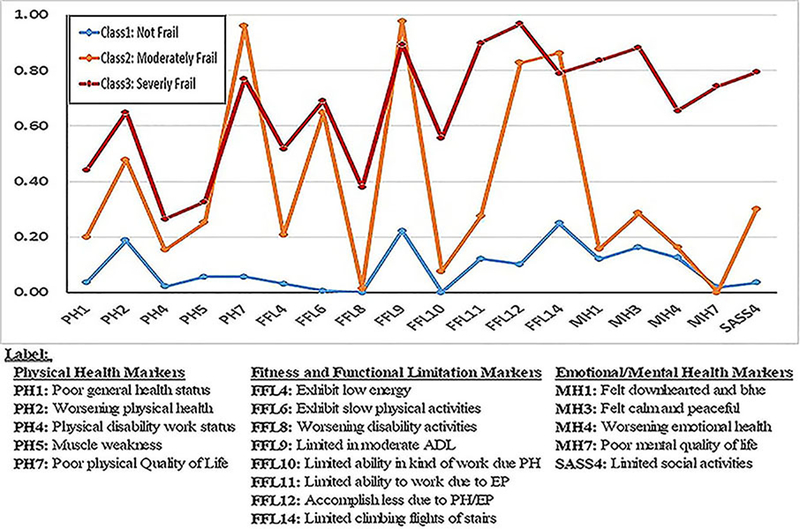
Results: The 18 markers provided psychometric evidence of a single reliable continuum of frailty severity. Latent class analyses produced 3 distinct subtypes, based on patients' endorsement probabilities of the frailty indicators: not frail (49.7%), moderately frail (33.5%), and severely frail (16.7%). Unlike the moderate class, severely frail endorsed emotional health problems in addition to physical burdens and functional limitations. Models adjusting for age, sex, type of anesthesia, and intraoperative factors indicated that severely frail (odds ratio, 1.89; 95% confidence interval, 1.42-2.50) and moderately frail patients (odds ratio, 1.31; 95% confidence interval, 1.03-1.67) both had higher odds of experiencing postoperative complications compared to not frail patients. In a 3-way comparison, a higher proportion of severely frail patients (10.7%) reported poorer quality of life after surgery compared to moderately frail (9.2%) and not frail (8.3%) patients (P < .001). There was no significant difference among these groups in proportions reporting hospital readmission (5.6%, 5.1%, and 3.8%, respectively; P = .067).
Conclusions: Self-report frailty items can accurately discern 3 distinct phenotypes differing in composition and their relations with surgical outcomes. Systematically assessing a wider set of domains including limitations in functional, emotional, and social activities can inform clinicians on what precipitates loss of physiological reserve and profoundly influences patients' lives. This information can help guide the current discussion on frailty and add meaningful clinical tools to the surgical practice.
Conflict of interest statement
All coauthors approved the final version of the manuscript, and all declare that they have no conflict of interest regarding the publication of this study.
Figures
References
-
- Fried LP, Tangen CM, Walston J, et al., Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci, 2001. 56(3): p. M146–56. - PubMed
-
- Hogan DB, MacKnight C, Bergman H, Steering Committee, C.I.o.F., and Aging, Models, definitions, and criteria of frailty. Aging Clin Exp Res, 2003. 15(3 Suppl): p. 1–29. - PubMed
-
- Rockwood K, What would make a definition of frailty successful? Age & Ageing, 2005. 34(5): p. 432–4. - PubMed
-
- Abellan van Kan G, Rolland YM, Morley JE, and Vellas B, Frailty: toward a clinical definition. Journal of the American Medical Directors Association, 2008. 9(2): p. 71–2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
