

Rhabdomyolysis revisited: Detailed analysis of magnetic resonance imaging findings and their correlation with peripheral neuropathy
- PMID: 30113478
- PMCID: PMC6113046
- DOI: 10.1097/MD.0000000000011848
Rhabdomyolysis revisited: Detailed analysis of magnetic resonance imaging findings and their correlation with peripheral neuropathy
Abstract
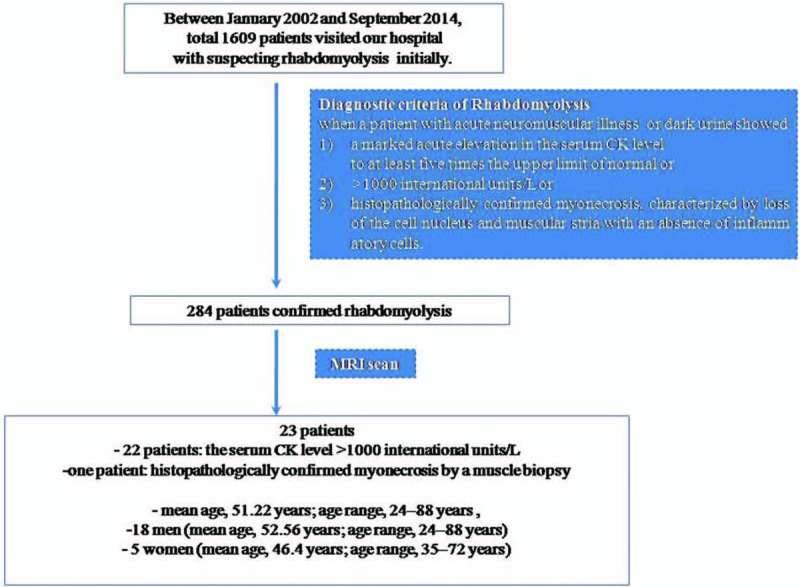
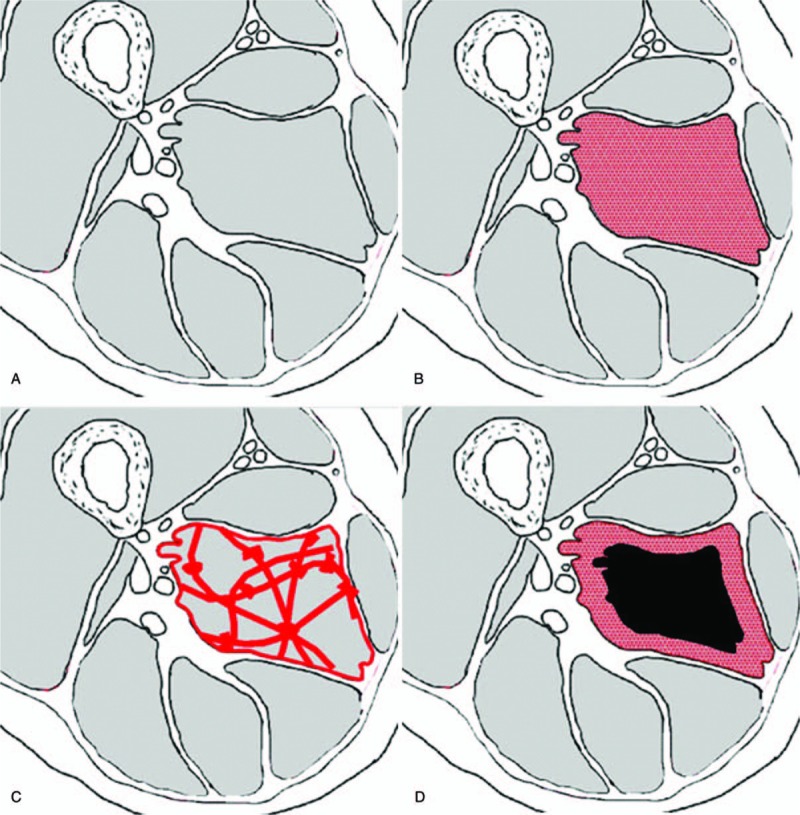
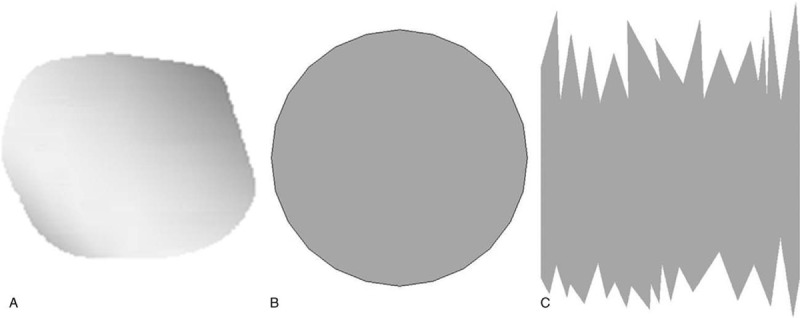
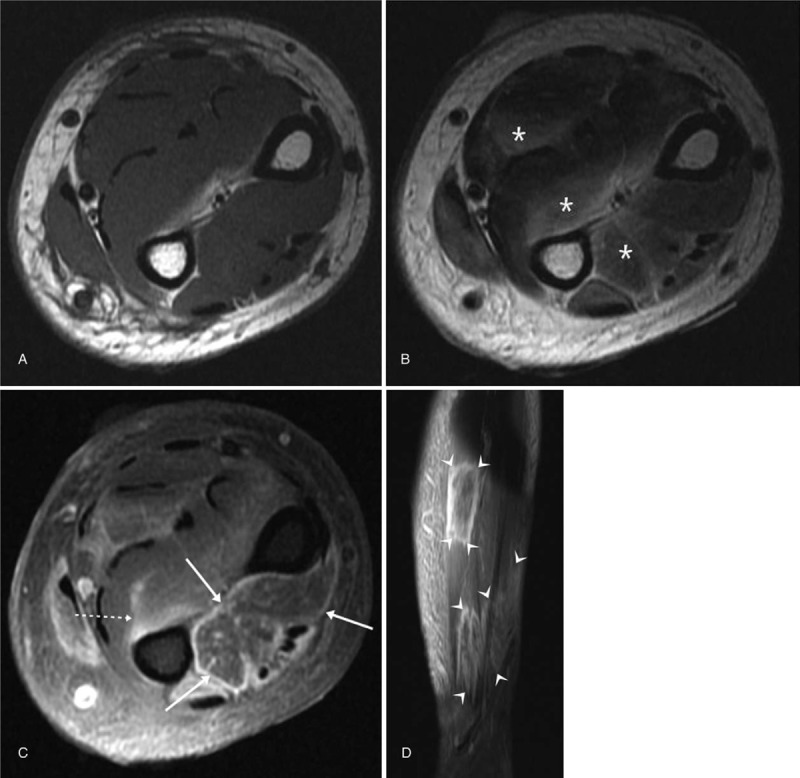
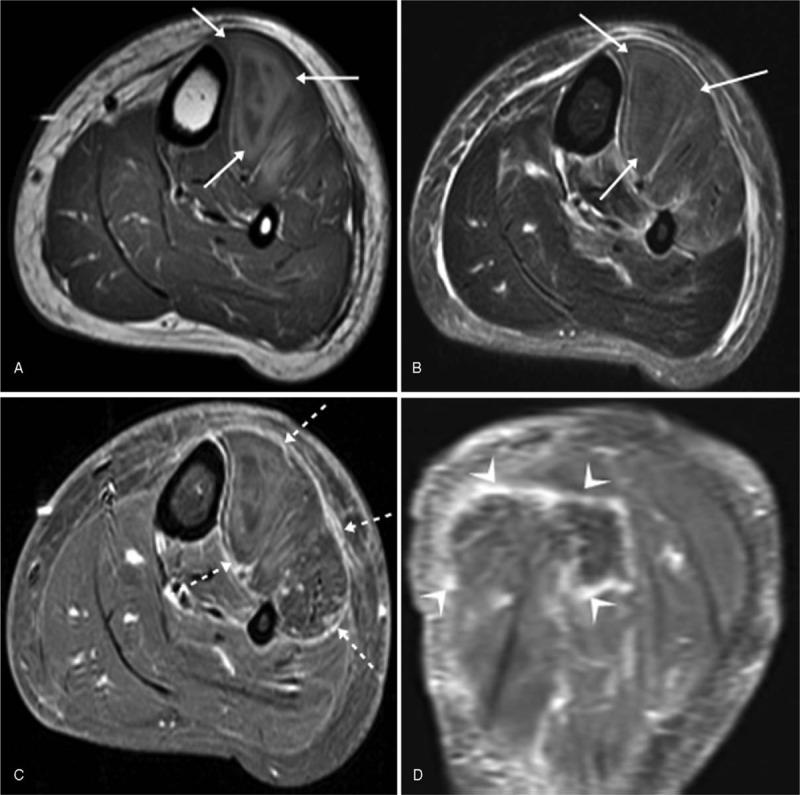
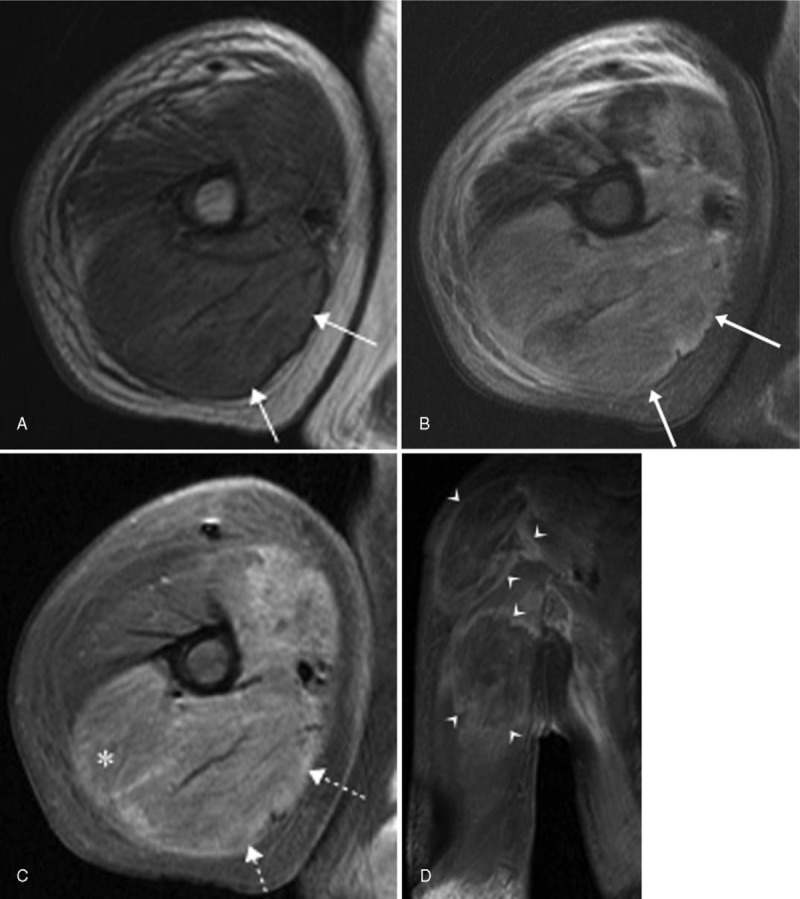
The objective is to evaluate the magnetic resonance imaging (MRI) findings in rhabdomyolysis in detail and determine their correlation with the development of peripheral neuropathy.Magnetic resonance images for 23 patients with confirmed rhabdomyolysis with (n = 11) or without (n = 12) peripheral neuropathy were retrospectively reviewed for the signal intensity on T1- and T2-weighted images, intramuscular hemorrhage, enhancement pattern, shape and margin in the longitudinal plane, edema in the deep fascia and overlying subcutaneous layer, multiplicity, and bilateral limb involvement. The collected data were statistically analyzed and the relationship between the imaging findings and the development of peripheral neuropathy was determined.Abnormal signal intensities on T1- or T2-weighted images were observed for all patients except one. Fourteen patients (60.9%) showed intramuscular hemorrhage. Stippled enhancement (11/23; 47.8%) was the most common enhancement pattern. Nineteen patients (86.4%) showed a well-defined rectangular shape with a ragged margin in the longitudinal plane. The affected muscle volume usually increased (17/23; 73.9%), with edema in the deep fascia and the overlying subcutaneous layer (13/23; 56.5%). Multiplicity within a muscle, compartment, and limb was observed in 7 (31.8%), 18 (81.8%), and 16 (72.7%) patients, respectively. Bilateral involvement was observed in 7 patients (30.4%). Only multiplicity within a compartment showed a statistically significant correlation with peripheral neuropathy development.Common MRI findings in rhabdomyolysis include intramuscular hemorrhage, stippled enhancement, a well-defined rectangular shape with a ragged margin in the longitudinal plane, and multiplicity. Multiplicity within a compartment may be a predictor of the development of peripheral neuropathy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Thomas MA, Ibels LS. Rhabdomyolysis and acute renal failure. Aust N Z J Med 1985;15:623–8. - PubMed
-
- McDonald S, Bearcroft P. Compartment syndromes. Semin MusculoskeletRadiol 2010;14:236–44. - PubMed
-
- Moratalla MB, Braun P, Fornas GM. Importance of MRI in the diagnosis and treatment of rhabdomyolysis. Eur J Radiol 2008;65:311–5. - PubMed
-
- Delaney-Sathy LO, Fessell DP, Jacobson JA, et al. Sonography of diabetic muscle infarction with MR imaging, CT, and pathologic correlation. AJR Am J Roentgenol 2000;174:165–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
