

Associations of Intensive Care Unit Capacity Strain with Disposition and Outcomes of Patients with Sepsis Presenting to the Emergency Department
- PMID: 30113865
- PMCID: PMC6850726
- DOI: 10.1513/AnnalsATS.201804-241OC
Associations of Intensive Care Unit Capacity Strain with Disposition and Outcomes of Patients with Sepsis Presenting to the Emergency Department
Abstract
Rationale: Intensive care unit (ICU) capacity strain refers to the potential limits placed on an ICU's ability to provide high-quality care for all patients who may need it at a given time. Few studies have investigated how fluctuations in ICU capacity strain might influence care outside the ICU.
Objectives: To determine whether ICU capacity strain is associated with initial level of inpatient care and outcomes for emergency department (ED) patients hospitalized for sepsis.
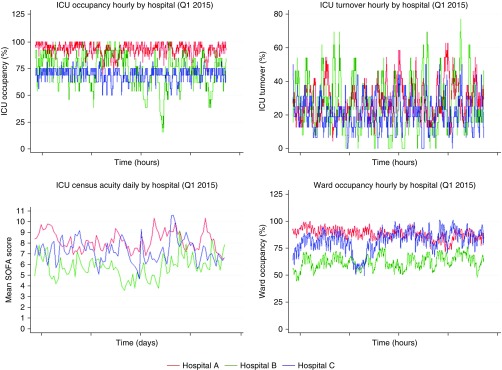
Methods: We performed a retrospective cohort study of patients with sepsis admitted from the ED to a medical ward or ICU at three hospitals within the University of Pennsylvania Health System between 2012 and 2015. Patients were excluded if they required life support therapies, defined as invasive or noninvasive ventilatory support or vasopressors, at the time of admission. The exposures were four measures of ICU capacity strain at the time of the ED disposition decision: ICU occupancy, ICU turnover, ICU census acuity, and ward occupancy. The primary outcome was the decision to admit to a ward or to an ICU. Secondary analyses assessed the association of ICU capacity strain with in-hospital outcomes, including mortality.
Results: Among 77,142 hospital admissions from the ED, 3,067 patients met the study's eligibility criteria. The ICU capacity strain metrics varied between and within study hospitals over time. In unadjusted analyses, ICU occupancy, ICU turnover, ICU census acuity, and ward occupancy were all negatively associated with ICU admission. In the fully adjusted model including patient-level covariates, only ICU occupancy remained associated with ICU admission (odds ratio, 0.87; 95% confidence interval, 0.79-0.96; P = 0.005), such that a 10% increase in ICU occupancy (e.g., one additional patient in a 10-bed ICU) was associated with a 13% decrease in the odds of ICU admission. Among the subset of patients admitted initially from the ED to a medical ward, ICU occupancy at the time of admission was associated with increased odds of hospital mortality (odds ratio, 1.61; 95% confidence interval, 1.21-2.14; P = 0.001).
Conclusions: The odds that patients in the ED with sepsis who do not require life support therapies will be admitted to the ICU are reduced when those ICUs experience high occupancy but not high levels of other previously explored measures of capacity strain. Patients with sepsis admitted to the wards during times of high ICU occupancy had increased odds of hospital mortality.
Keywords: ICU occupancy; intensive care unit capacity strain; sepsis.
Figures


Comment in
-
The Search for the Optimal Intensive Care Unit Triage Model.Ann Am Thorac Soc. 2018 Nov;15(11):1280-1282. doi: 10.1513/AnnalsATS.201808-577ED. Ann Am Thorac Soc. 2018. PMID: 30382788 Free PMC article. No abstract available.
References
-
- Halpern SD. ICU capacity strain and the quality and allocation of critical care. Curr Opin Crit Care. 2011;17:648–657. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
