

Review
. 2018 Sep;159 Suppl 1(Suppl 1):S31-S42.
doi: 10.1097/j.pain.0000000000001301.
Using stratified medicine to understand, diagnose, and treat neuropathic pain
Affiliations
- PMID: 30113945
- PMCID: PMC6130809
- DOI: 10.1097/j.pain.0000000000001301
Item in Clipboard
Review
Using stratified medicine to understand, diagnose, and treat neuropathic pain
Pain.
2018 Sep.
No abstract available
Conflict of interest statement
DLB has undertaken consultancy and advisory board work for Oxford innovation—in the past 36 months, this has included work for Abide, Biogen, GSK, Lilly, Mitsubishi Tanabe, Mundipharma, Teva, and Pfizer.
Figures
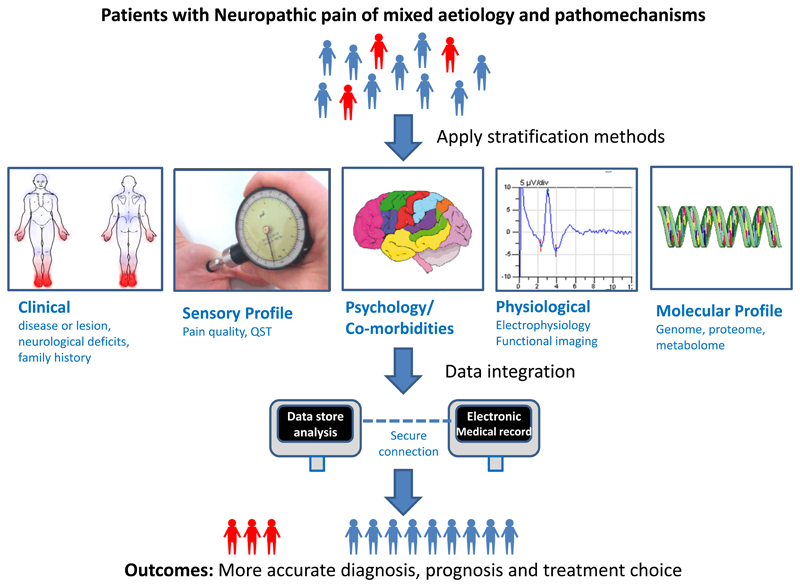
Schematic representation of some of the techniques that can be used to stratify neuropathic pain patients. Techniques to stratify patients in the context of neuropathic pain have been developed over the last decade. These include: detailed clinical assessment, psychophysical tools to assess sensory profiles; questionnaires to assess pain quality, pain severity, comorbidities and psychological impact; neurophysiological tools that can include nerve conduction studies, somatosensory evoked potentials and functional brain imaging; and, molecular profiling. Integration of data from diverse sources such as electronic health records, routine investigation and specialised investigations from biobank material, followed by downstream multivariate analysis provides a framework that will yield improvements in diagnosis, prognosis and treatment outcomes.
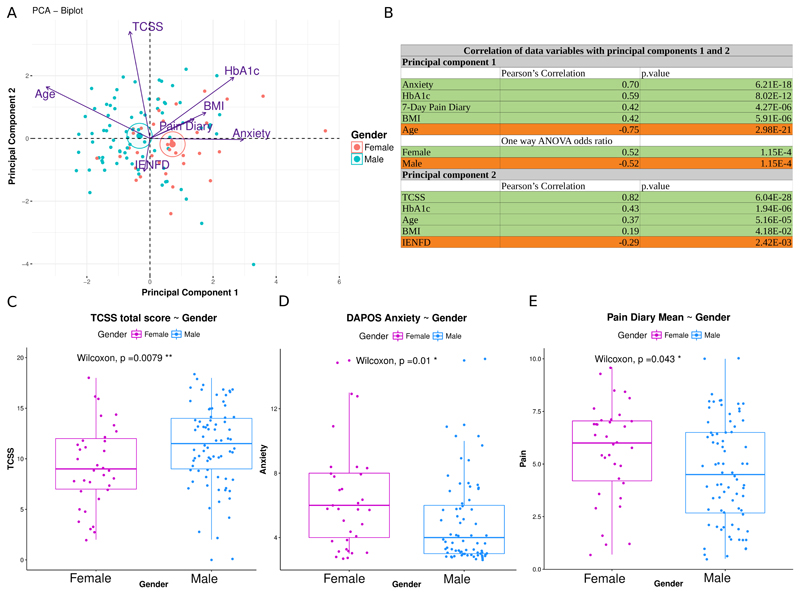
A: PCA biplot of individuals and variables based on the first 2 principal components in a cohort of patients with neuropathic pain secondary to diabetic neuropathy. Dots represent individuals projected on the 2-dimensional plot. Individuals are colour coded according to gender. Active variables used for constructing the components are projected on the 2-dimensional plot, with arrows proportional to the variable’s contribution to the principal component. Angles between variables (co-sinus) represent their correlation. Arrows pointing in opposite directions indicate negatively correlated variables, pointing in the same direction indicating positively correlated variables and perpendicular are the uncorrelated variables. Centroids of the groups are shown with large dots and ellipses. B: Correlation of original variables with the principal components. Pearson's R correlation coefficient is shown only when significant (p value < 0.05) for active continuous variables. Principal component’s association with the supplementary categorical variables “Male” and “Female” was calculated using one-way ANOVA. The first component (PC1) was strongly and significantly associated with anxiety, body mass index (BMI), high self-reported scores, younger age, and high HbA1c (glycosylated haemoglobin) and the second component (PC2) was associated with more severe neuropathy and low intra-epidermal nerve fibre density (IENFD) (Figure B). Principal component 1, was also significantly associated with females. The rows highlighted in green are for positively correlated variables. The rows highlighted in orange are for negatively correlated variables. C-E: Boxplots showing the median and the interquartile range for TCSS (Toronto Clinical Scoring System a measure of neuropathy severity) total score, DAPOS anxiety score and 7-Day pain diary mean score for males and females. The two-sided Mann-Whitney Wilcoxon rank sum test was used to compare groups. Males had significantly higher TCSS scores (Figure C) while women reported significantly higher anxiety (Figure D) and scores in the 7-Day pain diary (Figure E) (p value < 0.05 *, p value < 0.01 **). The analysis completed in this figure adopted the same techniques as applied in Sieberg et al. [76]. The current data was restricted to only those patients with neuropathic pain.
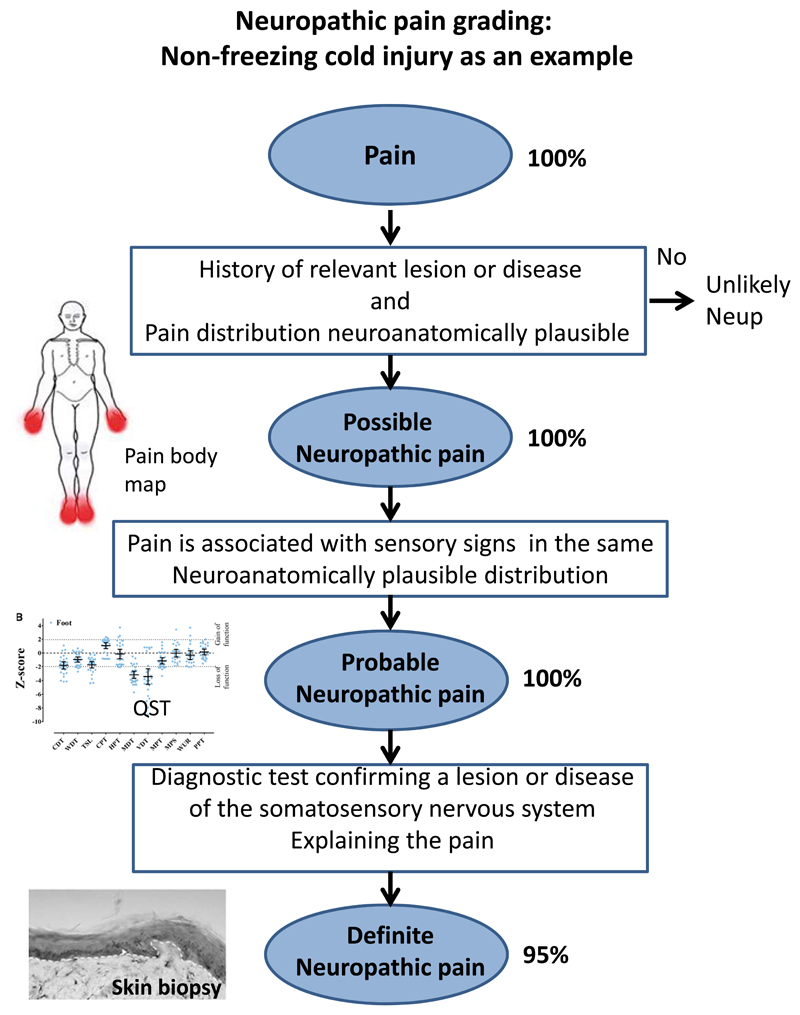
This provides an example of how detailed phenotyping and application of the NeupSIG grading system was applied to non-freezing cold injury. Non-freezing cold injury arises following exposure to a cold wet environment, most commonly in army service personnel. This condition is associated with disabling chronic pain but the basis of this pain remained mysterious. All study participants gave a history of exposure to a cold wet environment with acute onset of sensory symptoms (pain, numbness and paresthesia) that then persisted for at least 3 months. Pain was present symmetrically in the hands and feet (a body map is shown). Possible neuropathic pain was fulfilled in 100% of cases. Bed-side clinical sensory examination and quantitative sensory examination revealed sensory loss in the hands and feet and all subjects met criteria for probable neuropathic pain. Skin biopsy revealed reduced intra-epidermal nerve fibers confirming a lesion at structural level and 95% of study participants met criteria for definite neuropathic pain. Data used in figure derived from Vale et al., [92].
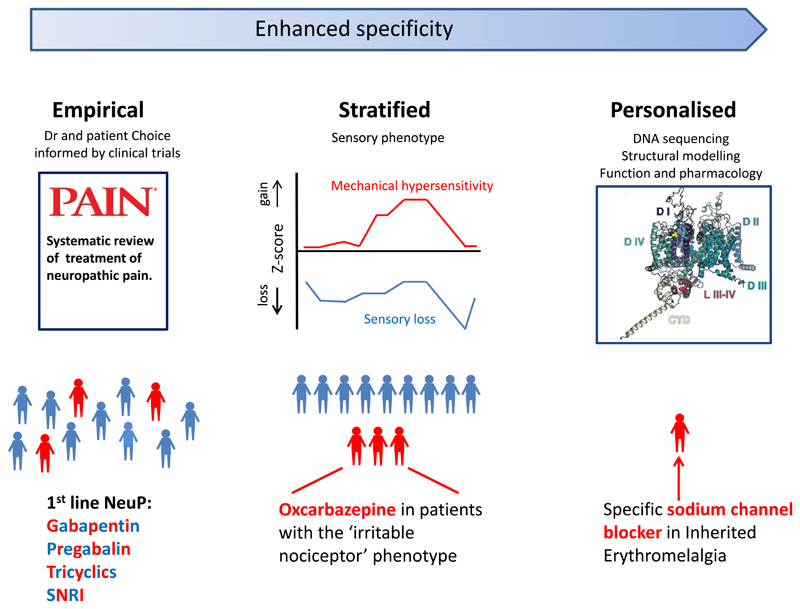
A schematic showing the continuum of improved targeting of pain therapies. Current first line agents for the treatment of neuropathic pain include: tricyclic antidepressants (eg. amitriptyline), dual serotonin and noradrenaline reuptake inhibitors (eg. duloxetine) and the Gabapentinoids (eg. pregabalin and gabapentin). Initial treatment selection is usually empirical and is not guided by predicted efficacy in individual patients. Sensory profiling is a stratification measure which may help target treatment. Patients with an “irritable nociceptor” phenotype, a profile with preserved small-fiber function together with hyperalgesia, obtain a greater analgesic response to oxcarbazepine than to placebo. The most specific and personalized treatments are based on the identification of genetic variants that are functionally responsive to specific drugs. Structural modelling of the ion channel (illustrated) can aid in predicting such a treatment response. The use of carbamazepine or mexiletine, which can normalize the gain of function effects in certain Nav1.7 mutations associated with inherited erythromelagia, is the prototypical example of such a personalized approach. SNRI- Serotonin and Noradrenaline Reuptake Inhibitors (Figure of sodium channel adapted with permission from Blesneac I, Themistocleous AC, Fratter C, Conrad LJ, Ramirez JD, Cox JJ, Tesfaye S, Shillo PR, Rice ASC, Tucker SJ, Bennett DLH. Rare NaV1.7 variants associated with painful diabetic peripheral neuropathy. Pain. 2018 Mar; 159(3):469-480. doi: 10.1097/j.pain.0000000000001116 , https://journals.lww.com/pain/fulltext/2018/03000/Rare_NaV1_7_variants_associated_with_painful.10.aspx )
References
-
- Attal N, Bouhassira D, Baron R. Diagnosis and assessment of neuropathic pain through questionnaires. The Lancet Neurology. 2018;17(5):456–466. - PubMed
-
- Attal N, de Andrade DC, Adam F, Ranoux D, Teixeira MJ, Galhardoni R, Raicher I, Uceyler N, Sommer C, Bouhassira D. Safety and efficacy of repeated injections of botulinum toxin A in peripheral neuropathic pain (BOTNEP): a randomised, double-blind, placebo-controlled trial. The Lancet Neurology. 2016;15(6):555–565. - PubMed
-
- Baron R, Forster M, Binder A. Subgrouping of patients with neuropathic pain according to pain-related sensory abnormalities: a first step to a stratified treatment approach. The Lancet Neurology. 2012;11(11):999–1005. - PubMed
-
- Baron R, Tölle TR, Gockel U, Brosz M, Freynhagen R. A cross-sectional cohort survey in 2100 patients with painful diabetic neuropathy and postherpetic neuralgia: Differences in demographic data and sensory symptoms. PAIN. 2009;146(1–2):34–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
