

Value-based evaluation of dialysis versus conservative care in older patients with advanced chronic kidney disease: a cohort study
- PMID: 30115028
- PMCID: PMC6097302
- DOI: 10.1186/s12882-018-1004-4
Value-based evaluation of dialysis versus conservative care in older patients with advanced chronic kidney disease: a cohort study
Abstract
Background: Conservative care is argued to be a reasonable treatment alternative for dialysis in older patients with advanced chronic kidney disease (CKD). However, comparisons are scarce and generally focus on survival only. Comparative data on more patient-relevant outcomes are needed to truly foster shared decision-making on an individual level, and cost comparison is needed to assess value of care.
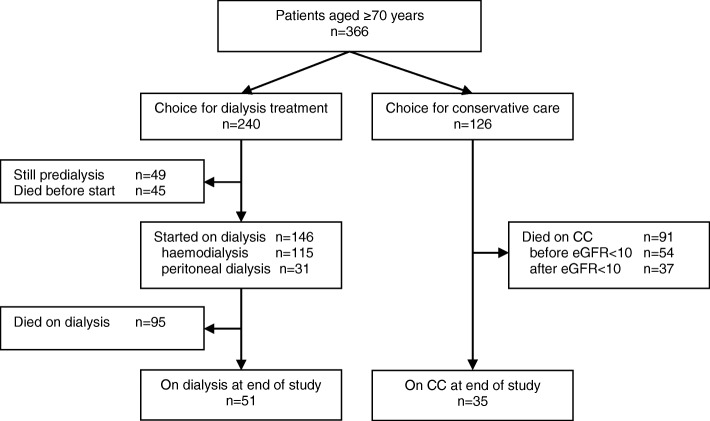
Methods: We conducted a retrospective observational single-center cohort study in 366 patients aged ≥70 years with advanced CKD, who chose dialysis (n = 240) or conservative care (n = 126) after careful counselling by a multidisciplinary team in a non-academic teaching hospital in The Netherlands. Using a value-based health care approach (value = outcomes/cost): survival, health-related quality of life-cross-sectionally assessed with the Kidney Disease Quality of Life Short Form™-treatment burden, and treatment costs were evaluated.
Results: The overall survival benefit of patients on a dialysis pathway compared with patients on conservative care diminished or lost significance in patients aged ≥80 years or with severe comorbidity. There were no differences between patients managed conservatively and dialysis patients on physical and mental health summary scores (all P > 0.1). Patients on conservative care had 352.7 hospital free days per year versus 282.7 in patients on a dialysis pathway, calculated from treatment decision (adjusted incidence rate ratio: 1.15, 95% confidence interval: 1.09 to 1.21, P < 0.001). Annual treatment costs were lower in patients on conservative care (adjusted cost ratio: 0.43, 95% confidence interval: 0.28 to 0.67, P < 0.001).
Conclusions: In this study, conservative care is shown to be a viable treatment option in older patients with advanced CKD, particularly in the oldest old and those with severe comorbidity. By achieving similar outcomes at lower treatment burden and treatment costs, value was generated for older patients choosing conservative care and society.
Keywords: Aged; Chronic kidney failure; Conservative treatment; End-stage renal disease (ESRD); Renal dialysis.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was obtained from the local research ethics committee (Verenigde Commissies Mensgebonden Onderzoek; reference W14.053). Informed written consent was obtained from patients prior to data collection.
Consent for publication
not applicable.
Competing interests
WV was research fellow of the International Consortium for Health Outcomes Measurement (ICHOM) Chronic Kidney Disease (CKD) Working Group. WB chaired the ICHOM CKD Working Group. All authors declare no financial conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Hoekstra T, Hemmelder M, Van Ittersum F. RENINE annual report 2015. Available from: http://www.nefrovisie.nl/wp-content/uploads/2017/03/RENINE-year-report_0.... Accessed 1 May 2017.
-
- Kallenberg MH, Kleinveld HA, Dekker FW, van Munster BC, Rabelink TJ, van Buren M, et al. Functional and cognitive impairment, frailty, and adverse health outcomes in older patients reaching ESRD-A systematic review. Clin J Am Soc Nephrol. 2016;11(9):1624–1639. doi: 10.2215/CJN.13611215. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
