

Preliminary clinical experience with robotic retroperitoneoscopic pancreatic surgery
- PMID: 30115072
- PMCID: PMC6097221
- DOI: 10.1186/s12957-018-1468-5
Preliminary clinical experience with robotic retroperitoneoscopic pancreatic surgery
Abstract
Backgrounds: Retroperitoneoscopic surgery has shown advantages in urological surgery. However, its application in pancreatic surgery for neoplasm is rare. Robotic surgical system with its magnified view and flexible instruments may provide a superior alternative to conventional laparoscopic system in retroperitoneoscopic surgery. We aimed to evaluate the safety, feasibility, and short-term outcomes in a series of patients treated by robotic retroperitoneoscopic pancreatic surgery.
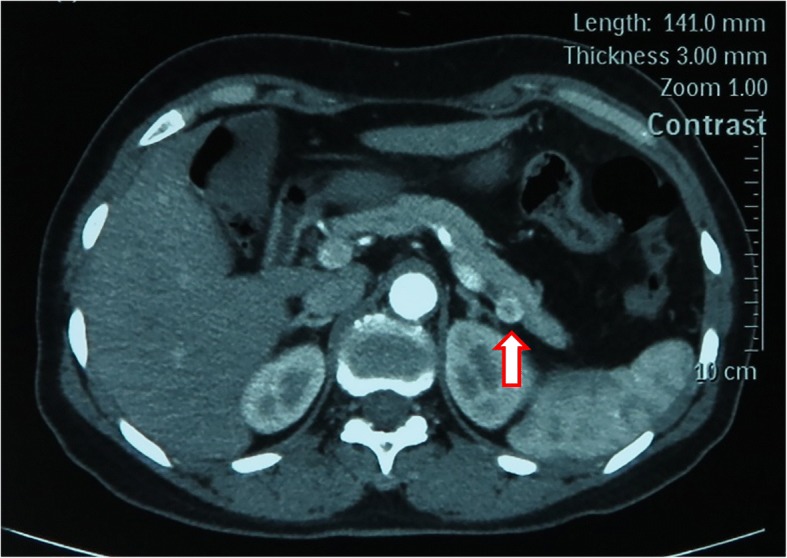
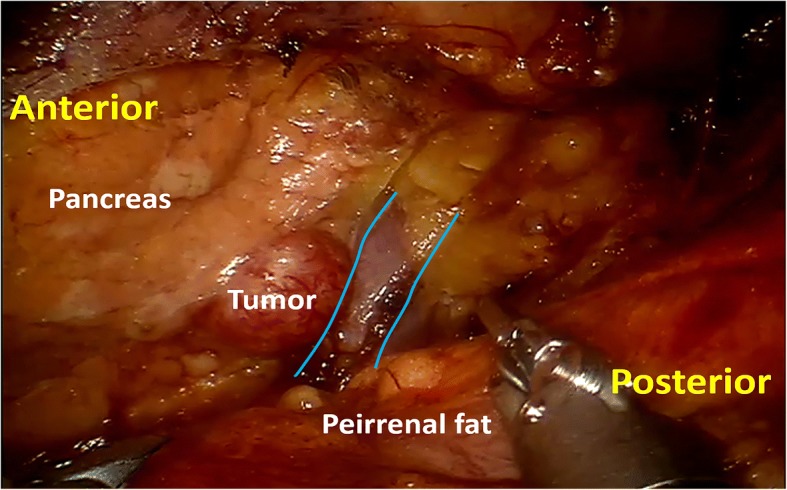
Case presentation: Between March 2016 and May 2016, four patients with solitary pancreatic neuroendocrine neoplasms were treated with robotic retroperitoneoscopic surgery. Prospective collected clinical data were retrospectively analyzed. Three patients underwent distal pancreatectomy (one combined with resection of left adrenal adenoma), and one patient enucleation. The mean operative time was 80 min (range 30-110 min). The estimated blood loss was insignificant. There was no conversion to open procedure. The mean postoperative hospital stay was 5.25 days (range 4-6 days). The mean tumor size was 1.375 cm (range 1.0-1.8 cm) in diameter. All patients' blood glucose level returned to normal range within 1 week postoperatively. Two patients had pancreatic biochemical leak. No patients underwent subsequent treatment, and no recurrence occurred during the 12-month follow-up period.
Conclusions: This study preliminarily indicates that robotic retroperitoneoscopic pancreatic surgery is safe and feasible for neoplasms in the dorsal portion of distal pancreas in selected patients, with some potential advantages of straightforward access, simple and fine manipulation, short operative time, and fast recovery.
Keywords: Distal pancreatectomy; Enucleation; Neoplasm; Pancreas; Retroperitoneoscopic surgery; Robotic surgery.
Conflict of interest statement
Ethics approval and consent to participant
Ethical approval for this medical study involving human subjects has respected the Helsinki ethical principles.
Consent for publication
Informed consent was obtained from the patients for the publication and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Robot-assisted posterior retroperitoneoscopic adrenalectomy using single-port access: technical feasibility and preliminary results.Ann Surg Oncol. 2013 Aug;20(8):2741-5. doi: 10.1245/s10434-013-2891-z. Epub 2013 Mar 14. Ann Surg Oncol. 2013. PMID: 23494081
-
Robotic single-site plus ONE port distal pancreatectomy.Surg Endosc. 2017 Oct;31(10):4258-4259. doi: 10.1007/s00464-017-5476-2. Epub 2017 Mar 24. Surg Endosc. 2017. PMID: 28342127
-
Retroperitoneoscopic pancreatectomy: a new surgical option for pancreatic disease.Surg Endosc. 2012 Jun;26(6):1609-16. doi: 10.1007/s00464-011-2078-2. Epub 2011 Dec 17. Surg Endosc. 2012. PMID: 22179465
-
Pre- and intraoperative diagnostic requirements, benefits and risks of minimally invasive and robotic surgery for neuroendocrine tumors of the pancreas.Best Pract Res Clin Endocrinol Metab. 2019 Oct;33(5):101294. doi: 10.1016/j.beem.2019.101294. Epub 2019 Jul 10. Best Pract Res Clin Endocrinol Metab. 2019. PMID: 31351817 Review.
-
Laparoscopic pancreatic surgery: current indications and surgical results.Surg Endosc. 2004 Mar;18(3):402-6. doi: 10.1007/s00464-003-8164-3. Epub 2004 Jan 23. Surg Endosc. 2004. PMID: 14735345 Review.
Cited by
-
Retroperitoneal totally endoscopic prosthetic repair of primary lumbar hernia.Hernia. 2021 Dec;25(6):1629-1634. doi: 10.1007/s10029-020-02334-z. Epub 2020 Nov 18. Hernia. 2021. PMID: 33206280
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
