

Epidemiology and patterns of tracheostomy practice in patients with acute respiratory distress syndrome in ICUs across 50 countries
- PMID: 30115127
- PMCID: PMC6097245
- DOI: 10.1186/s13054-018-2126-6
Epidemiology and patterns of tracheostomy practice in patients with acute respiratory distress syndrome in ICUs across 50 countries
Abstract
Background: To better understand the epidemiology and patterns of tracheostomy practice for patients with acute respiratory distress syndrome (ARDS), we investigated the current usage of tracheostomy in patients with ARDS recruited into the Large Observational Study to Understand the Global Impact of Severe Acute Respiratory Failure (LUNG-SAFE) study.
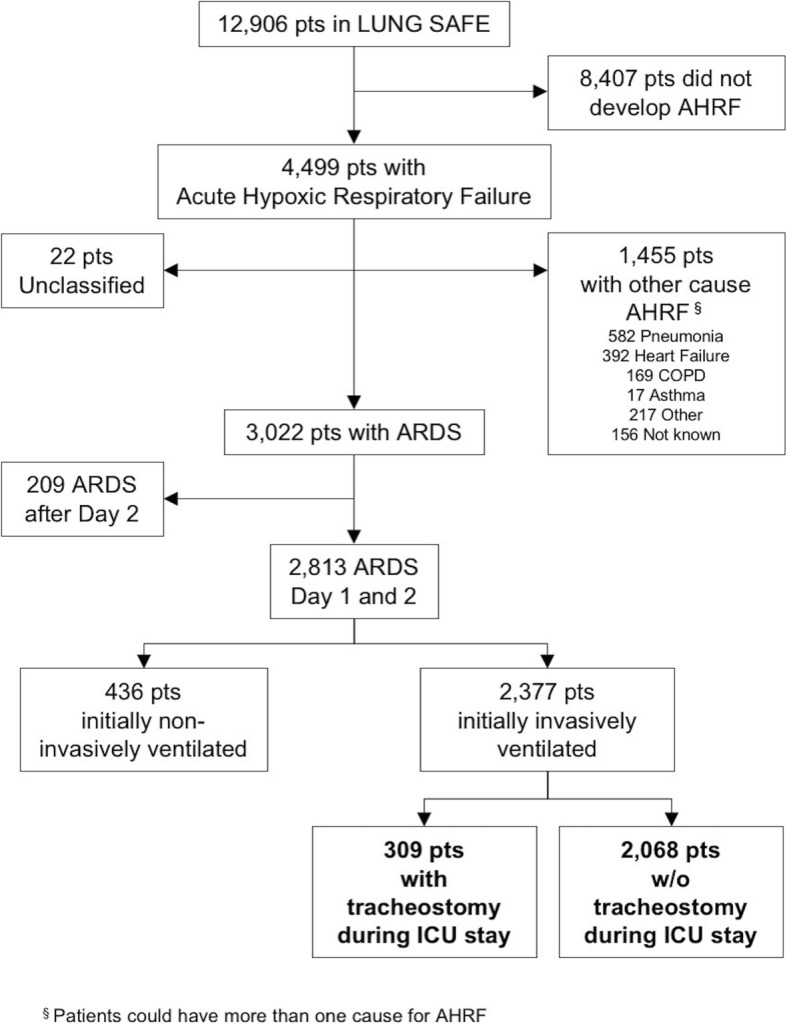
Methods: This is a secondary analysis of LUNG-SAFE, an international, multicenter, prospective cohort study of patients receiving invasive or noninvasive ventilation in 50 countries spanning 5 continents. The study was carried out over 4 weeks consecutively in the winter of 2014, and 459 ICUs participated. We evaluated the clinical characteristics, management and outcomes of patients that received tracheostomy, in the cohort of patients that developed ARDS on day 1-2 of acute hypoxemic respiratory failure, and in a subsequent propensity-matched cohort.
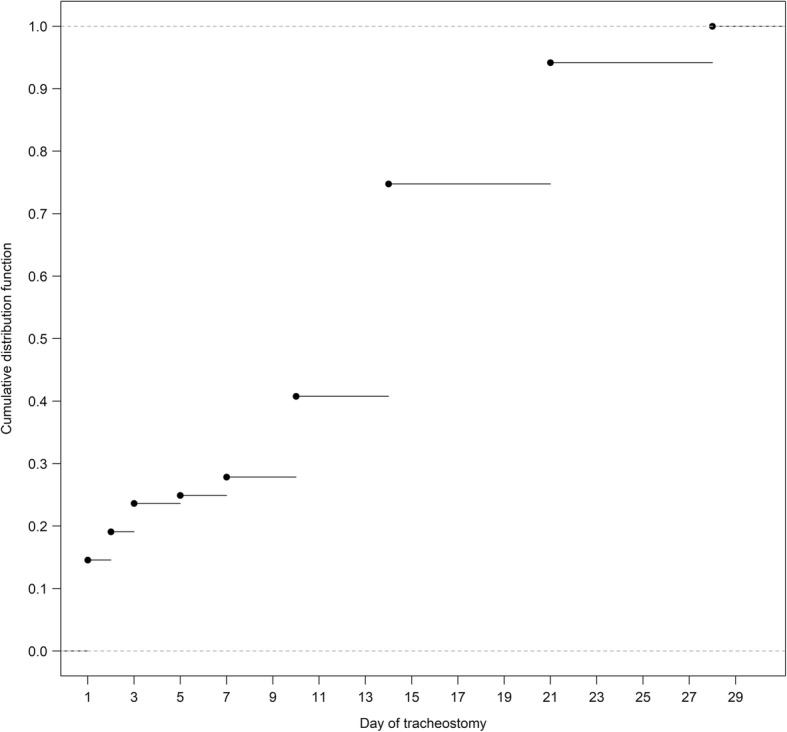
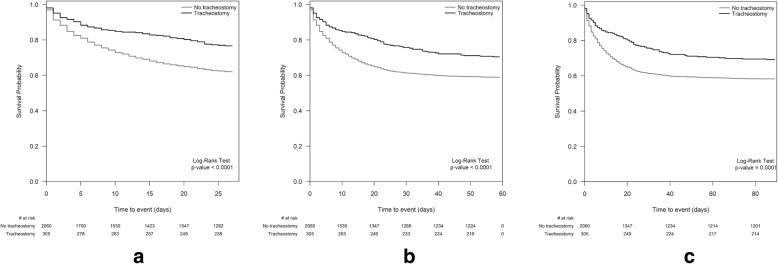
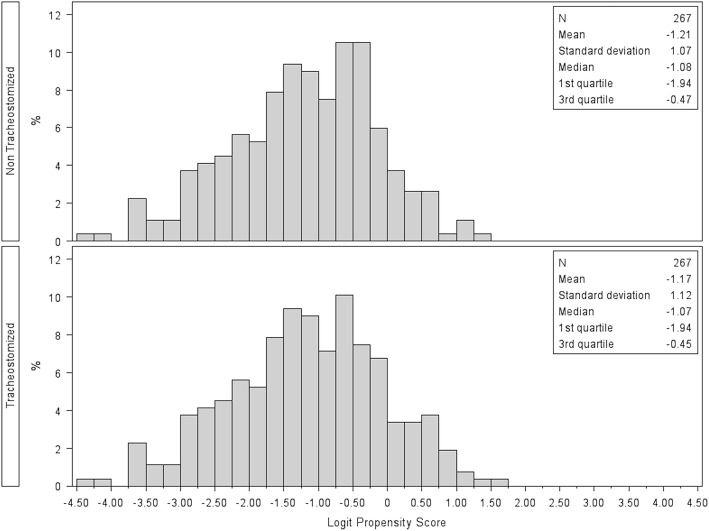
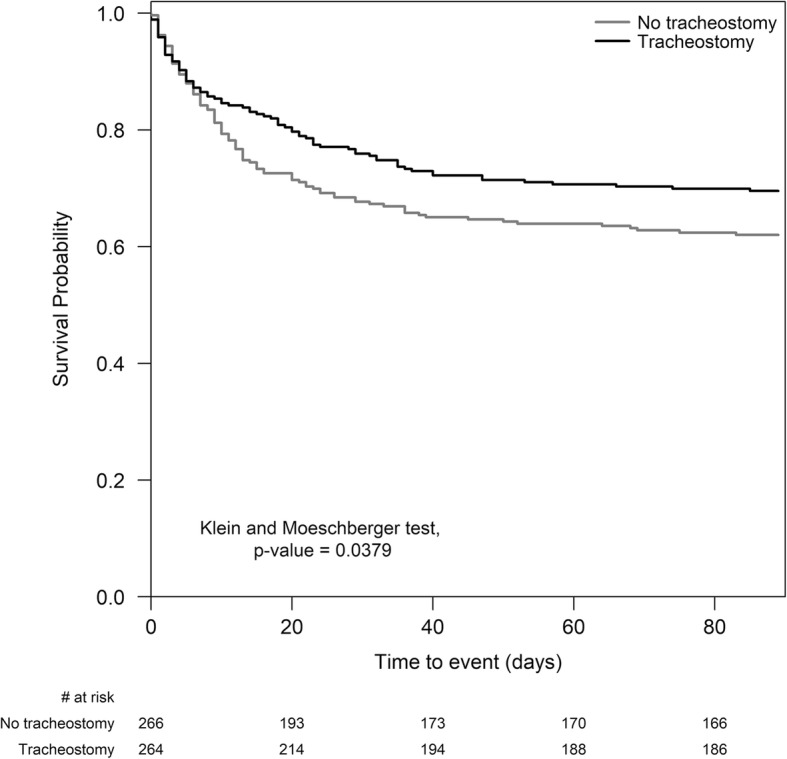
Results: Of the 2377 patients with ARDS that fulfilled the inclusion criteria, 309 (13.0%) underwent tracheostomy during their ICU stay. Patients from high-income European countries (n = 198/1263) more frequently underwent tracheostomy compared to patients from non-European high-income countries (n = 63/649) or patients from middle-income countries (n = 48/465). Only 86/309 (27.8%) underwent tracheostomy on or before day 7, while the median timing of tracheostomy was 14 (Q1-Q3, 7-21) days after onset of ARDS. In the subsample matched by propensity score, ICU and hospital stay were longer in patients with tracheostomy. While patients with tracheostomy had the highest survival probability, there was no difference in 60-day or 90-day mortality in either the patient subgroup that survived for at least 5 days in ICU, or in the propensity-matched subsample.
Conclusions: Most patients that receive tracheostomy do so after the first week of critical illness. Tracheostomy may prolong patient survival but does not reduce 60-day or 90-day mortality.
Trial registration: ClinicalTrials.gov, NCT02010073 . Registered on 12 December 2013.
Keywords: Acute respiratory distress syndrome (ARDS); ICU; Propensity-matched analysis; Tracheostomy; Ventilation.
Conflict of interest statement
Ethics approval and consent to participate
All participating ICUs obtained ethics committee approval and obtained either patient consent or ethics committee waiver of consent in the LUNG-SAFE study. The study protocol was also reviewed and approved by the ethics committee of Mito Kyodo General Hospital, University of Tsukuba Hospital Mito Medical Center, Japan.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Jaeger JM, Littlewood KA, Durbin CG., Jr The role of tracheostomy in weaning from mechanical ventilation. Respir Care. 2002;47(4):469–480. - PubMed
-
- Laffey JG, Bellani G, Pham T, Fan E, Madotto F, Bajwa EK, Brochard L, Clarkson K, Esteban A, Gattinoni L, et al. Potentially modifiable factors contributing to outcome from acute respiratory distress syndrome: the LUNG SAFE study. Intensive Care Med. 2016;42(12):1865–1876. doi: 10.1007/s00134-016-4571-5. - DOI - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
