

MRI Findings in Tumefactive Demyelinating Lesions: A Systematic Review and Meta-Analysis
- PMID: 30115676
- PMCID: PMC7655270
- DOI: 10.3174/ajnr.A5775
MRI Findings in Tumefactive Demyelinating Lesions: A Systematic Review and Meta-Analysis
Abstract
Background: Accurate diagnosis of tumefactive demyelinating lesions is clinically important to avoid unnecessary invasive biopsy or inappropriate treatment.
Purpose: We aimed to evaluate conventional and advanced MR imaging findings of tumefactive demyelinating lesions and determine the diagnostic performance of MR imaging for differentiating tumefactive demyelinating lesions from primary brain tumor.
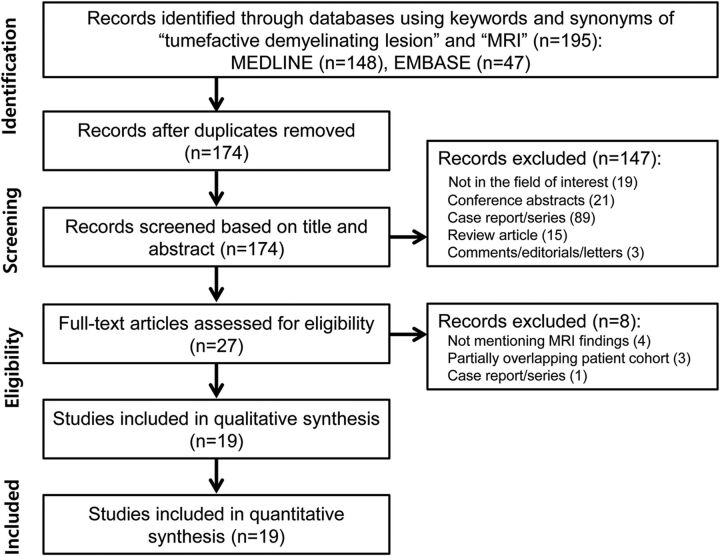
Data sources: A systematic search of Ovid MEDLINE and EMBASE up to December 6, 2017, was conducted.
Study selection: Original articles describing MR imaging findings in patients with tumefactive demyelinating lesions were selected.
Data analysis: The pooled incidences of conventional MR imaging findings of tumefactive demyelinating lesions were obtained with the DerSimonian and Liard random-effects model. The pooled sensitivity and specificity of MR imaging for differentiating tumefactive demyelinating lesions from primary brain tumor were obtained using the bivariate random-effects model.
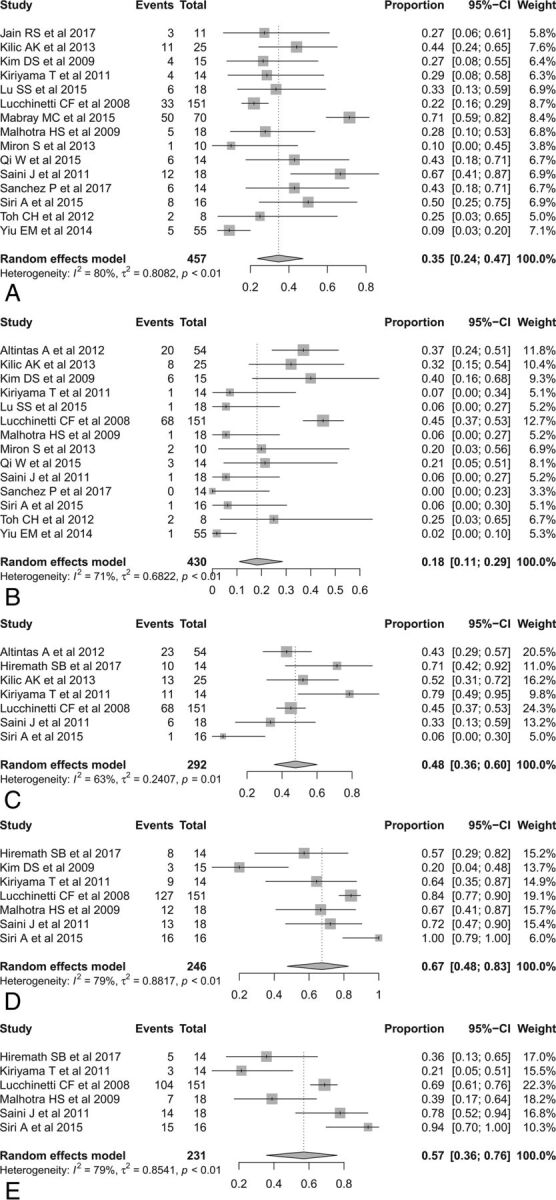
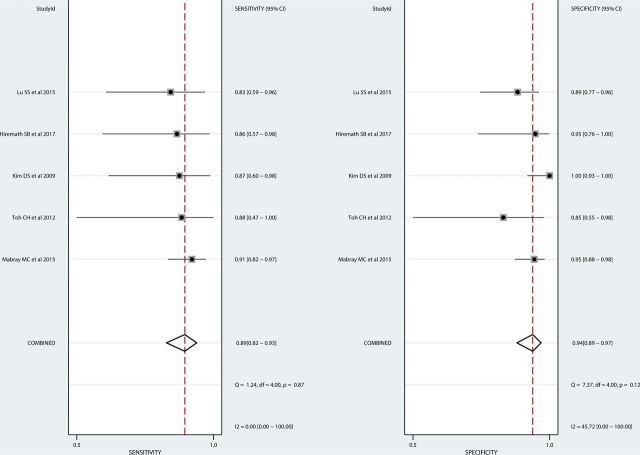
Data synthesis: Nineteen eligible studies with 476 patients with tumefactive demyelinating lesions were included. The pooled incidence of open ring or incomplete rim enhancement was 35% (95% CI, 24%-47%), which was significantly higher than the incidence of closed ring or complete rim enhancement (18% [95% CI, 11%-29%]; P = .0281). The pooled incidences of T2 hypointense rim, absent or mild mass effect, and absent or mild perilesional edema were 48%, 67%, and 57%, respectively. On advanced MR imaging, tumefactive demyelinating lesions showed a high apparent diffusion coefficient, peripheral restricted diffusion, and low cerebral blood volume. The pooled sensitivity and specificity of MR imaging for differentiating tumefactive demyelinating lesions from primary brain tumor were 89% (95% CI, 82%-93%) and 94% (95% CI, 89%-97%), respectively.
Limitations: Seventeen of 19 studies were retrospective studies.
Conclusions: Conventional MR imaging findings may help differentiate tumefactive demyelinating lesions from primary brain tumor, though further study is needed to determine the added value of advanced MR imaging.
© 2018 by American Journal of Neuroradiology.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical