

A prospective phase II study of pre-operative chemotherapy then short-course radiotherapy for high risk rectal cancer: COPERNICUS
- PMID: 30116024
- PMCID: PMC6173784
- DOI: 10.1038/s41416-018-0209-4
A prospective phase II study of pre-operative chemotherapy then short-course radiotherapy for high risk rectal cancer: COPERNICUS
Abstract
Background: Neoadjuvant chemotherapy (NAC) allows earlier treatment of rectal cancer micro-metastases but is not standard of care. There are currently no biomarkers predicting long-term progression-free survival (PFS) benefit from NAC.
Patients and methods: In this single arm phase II trial, patients with non-metastatic magnetic resonance imaging (MRI)-defined operable rectal adenocarcinoma at high risk of post-operative metastatic recurrence, received 8 weeks of oxaliplatin/fluorouracil NAC then short-course preoperative radiotherapy (SCPRT) before immediate surgery. Sixteen weeks of post-operative adjuvant chemotherapy (AC) was planned. A pelvic MRI was performed at week 9 immediately post-NAC, before SCPRT. The primary end point was feasibility assessed by completion of protocol treatment up to and including surgery. Secondary endpoints included compliance, toxicity, downstaging efficacy, and PFS.
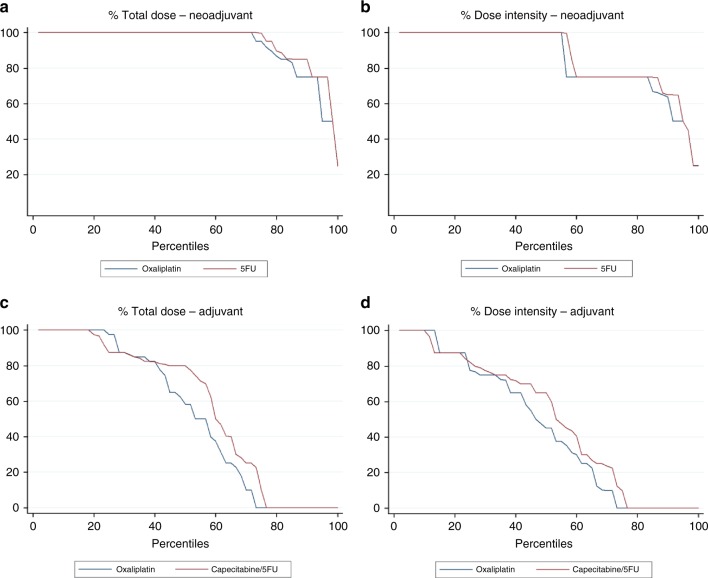
Results: In total 60 patients were recruited May 2012-June 2014. In total 57 patients completed protocol treatment, meeting the primary endpoint. Compliance with NAC was much better than AC: Comparing NAC vs. AC, the median percentage dose intensity for fluoropyrimidine was 100% vs. 63% and for oxaliplatin 100% vs. 45%. Treatment-related toxicity was acceptable with no treatment-related deaths. Post-NAC MRI showed 44 tumours (73%) were T-downstaged and 22 (37%) had excellent MRI tumour regression grade (mrTRG 1-2). Median follow-up was 27 months with 2-year PFS of 86.2% (10 events). On exploratory analysis, post-NAC mrTRG predicted PFS with no event among those with excellent regression.
Conclusion: The regimen was well tolerated with effective downstaging and encouraging PFS. mrTRG response to NAC may be a new prognostic factor for long-term PFS, but needs validation in larger studies.
Conflict of interest statement
Outside of the submitted work S.G. has received research funding from Roche and Pfizer. N.W. reports grants from Yorkshire Cancer Research, grants from Pathological Society of Great Britain and Ireland, during the conduct of the study; grants from Academy of Medical Sciences, grants from Cancer Research UK, outside the submitted work. N.B. reports speaking fees from Pfizer, and travel/accommodation support from Roche. P.Q. reports personal fees and research funding from Amgen, personal fees and research funding from Roche, research funding from Ventana, during the conduct of the study; grants from Yorkshire Cancer Research programme grant, within and outside the submitted work and grants from Cancer Research UK, outside the submitted work. R.A. has received research funding from Cancer Research UK, personal fees and travel from Merck Serono, Amgen and Servier.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
